
Autonomic Nervous System Drugs — MCQs

On this page
What is the most predictive and dangerous side effect of propranolol that makes it to be avoided in a known patient of COPD?
Choline esters like carbachol are most likely to cause which of the following adverse effects?
What is the effect of cocaine on blood vessels?
Dale's vasomotor reversal phenomenon occurs with which of the following?
A 32-year-old woman had abdominal surgery, after which she complains about difficulty in urination. Cholinomimetic stimulation with bethanechol or neostigmine is beneficial in relieving post-operative urinary retention. Neostigmine and bethanechol in moderate doses are likely to have different effects on what?
Intravenous administration of norepinephrine in a patient already taking an effective dose of atropine will often:
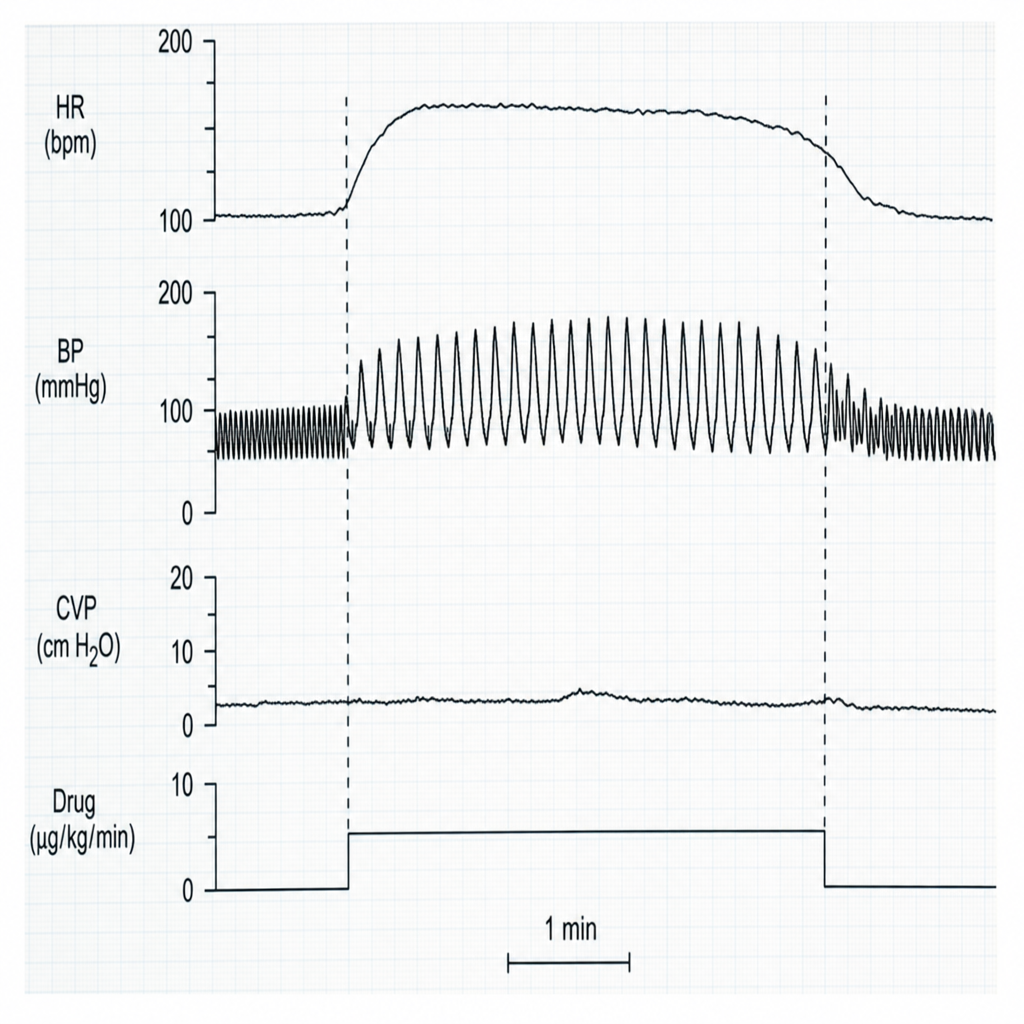
The unknown drug is likely to be:
Phase II block is seen in which of the following agents?
Carvedilol is an effective antihypertensive agent that, like propranolol, is capable of blocking beta receptors. An important difference between the two drugs is that carvedilol
All the following drugs are used in the management of pheochromocytoma except?
Practice by Chapter
Cholinergic Agonists
Practice Questions
Cholinergic Antagonists
Practice Questions
Adrenergic Agonists
Practice Questions
Adrenergic Antagonists
Practice Questions
Ganglionic Agents
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Autonomic Drugs in Ophthalmology
Practice Questions
Autonomic Drugs in Cardiovascular Disease
Practice Questions
Autonomic Drugs in Respiratory Disease
Practice Questions
Autonomic Drugs in Urological Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app