
Autonomic Nervous System Drugs — MCQs

On this page
Which drug used for the common cold can cause stroke?
All of the following drugs cause hypertensive crisis in patients with pheochromocytoma, EXCEPT:
Which antiglaucoma drugs are safe to use in a patient with asthma?
All of the following conditions are contraindicated or likely to cause issues in a patient treated with Timolol maleate 0.5% eye drops for Primary Open Angle glaucoma, EXCEPT:
Metoprolol is preferred over propranolol in some patients because it:
Propranolol is useful in the treatment of all of the following EXCEPT:
Which anti-adrenergic drug crosses the blood-brain barrier minimally?
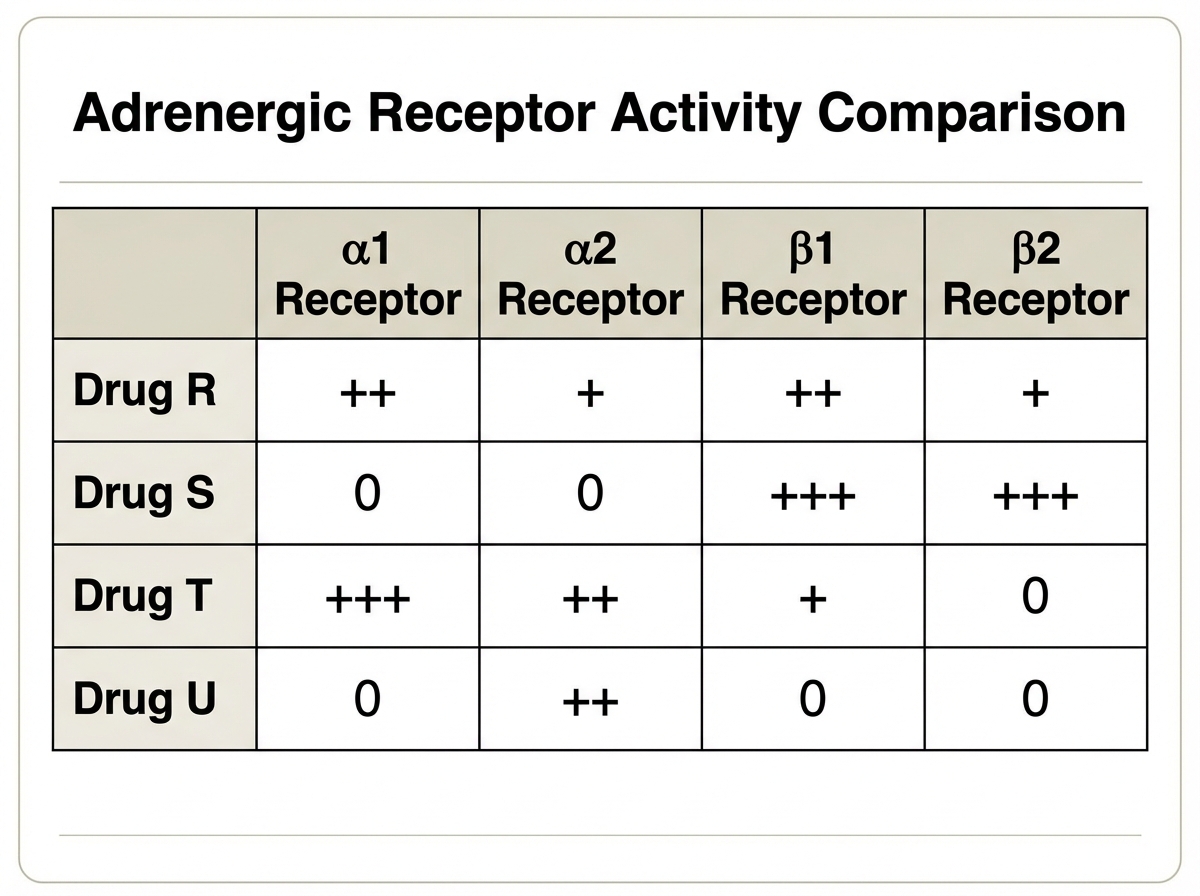
Drug S is most like which of the following drugs?
Which of the following is the earliest and shortest acting skeletal muscle relaxant?
The action of non-competitive muscle blockers is affected by which of the following?
Practice by Chapter
Cholinergic Agonists
Practice Questions
Cholinergic Antagonists
Practice Questions
Adrenergic Agonists
Practice Questions
Adrenergic Antagonists
Practice Questions
Ganglionic Agents
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Autonomic Drugs in Ophthalmology
Practice Questions
Autonomic Drugs in Cardiovascular Disease
Practice Questions
Autonomic Drugs in Respiratory Disease
Practice Questions
Autonomic Drugs in Urological Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app