
Autonomic Nervous System Drugs — MCQs

On this page
A gardener was accidentally poisoned by a weed killer that inhibits acetylcholinesterase. Which of the following alterations in neurochemical transmission at brain cholinergic synapses is the most likely result of this poisoning?
The regional aerial resistance of the mesentery and kidney is reduced by:
Neostigmine antagonizes non-depolarizing blockade by all of the following mechanisms EXCEPT:
What is the action of alpha 2 and beta 1 receptors on adenyl cyclase?
The use of succinylcholine is not contraindicated in which of the following conditions?
Therapeutic use of acetylcholine is not possible because it is -
Botulinum toxin mimics which class of drugs?
Which of the following is an example of a long-acting neuromuscular blocker?
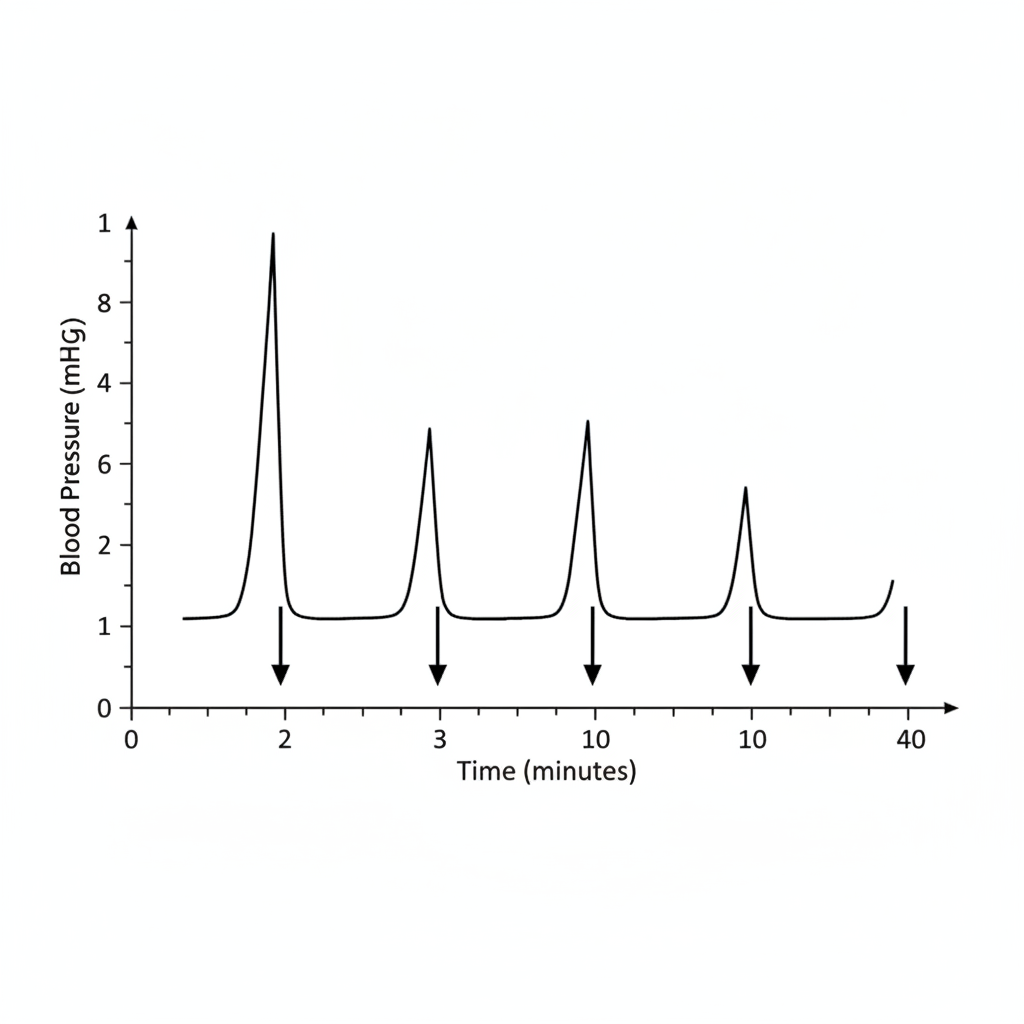
Vasomotor reversal of Dale is demonstrated by
Which of the following drugs exhibits the phenomenon described?
Practice by Chapter
Cholinergic Agonists
Practice Questions
Cholinergic Antagonists
Practice Questions
Adrenergic Agonists
Practice Questions
Adrenergic Antagonists
Practice Questions
Ganglionic Agents
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Autonomic Drugs in Ophthalmology
Practice Questions
Autonomic Drugs in Cardiovascular Disease
Practice Questions
Autonomic Drugs in Respiratory Disease
Practice Questions
Autonomic Drugs in Urological Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app