
Ganglionic Agents — MCQs

Acetylcholine acting on nicotinic receptors produces:
Ocular effects that include mydriasis are characteristic of which of the following drugs?
Which of the following is the most appropriate treatment for severe nicotine poisoning?
Which of the following neurotransmitters is primarily released from the sympathetic nervous system to increase heart rate in response to a DECREASE in blood pressure?
A chronic smoker wants to quit smoking. Which of the following is the MOST appropriate first-line pharmacotherapy for smoking cessation?
Which of the following is not a recognized use of alpha-2-agonists?
A 20-year-old woman is admitted with the following presentation. 1% pilocarpine is not showing any response on the side of mydriasis. What is the diagnosis? (Recent NEET Pattern 2016-17)
Empirical drug of choice for treatment of meningococcal meningitis is:-
Mechanism of action of atropine in treatment of organophosphate poisoning is?
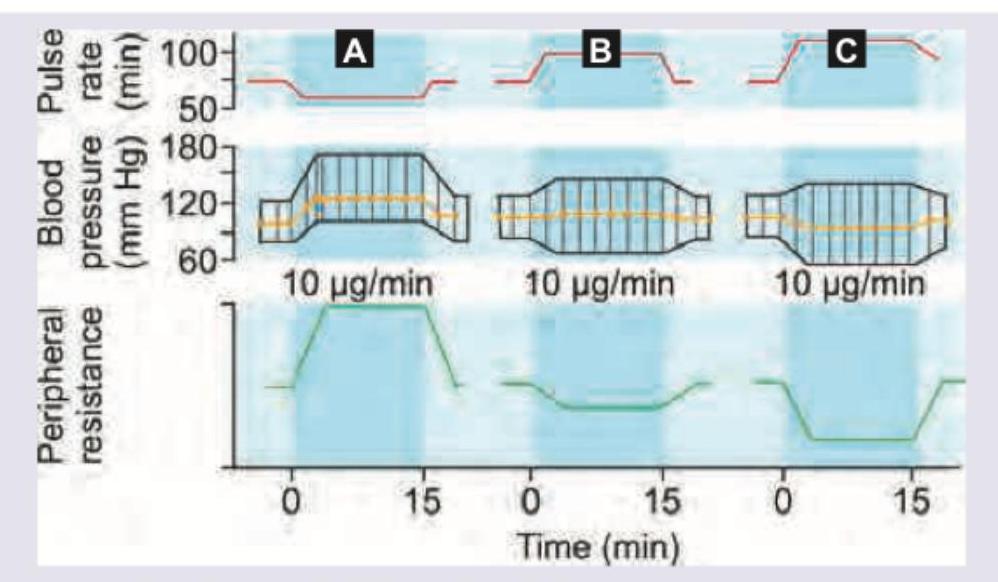
Which of the following statement is correct regarding the graph shown? (AllMS Nov 2016)
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app