
Neurology — MCQs

On this page
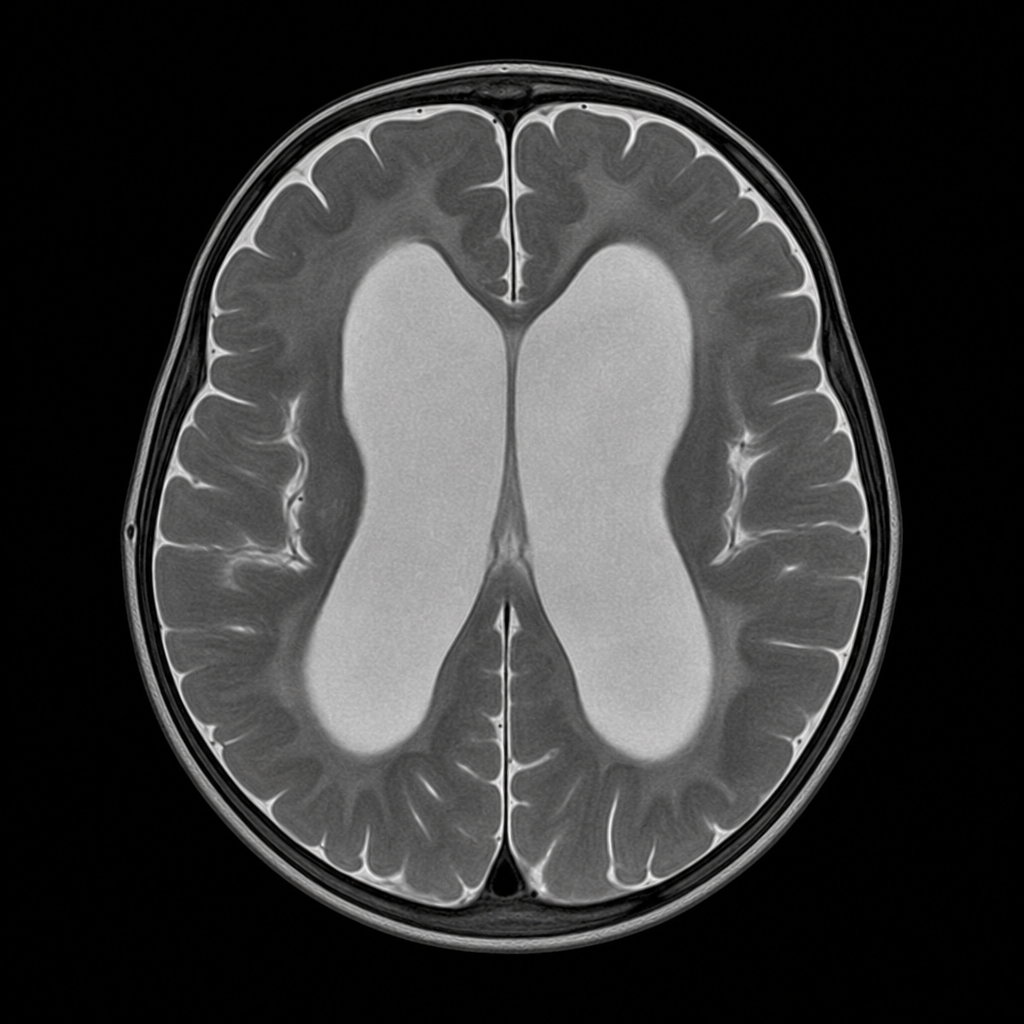
An infant presented with mental retardation, regression of motor skills, problems with feeding, impaired head control, and macrocephaly. MRI of the infant is shown below. What is the most probable diagnosis?
A 9-year-old boy presents with a several-day history of progressive arm and leg weakness. He had an upper respiratory infection two weeks prior to presentation. The patient is alert and oriented. On repeated examination, the heart rate varies between 60 and 140 beats/minute and the blood pressure varies between 90/60 and 140/90 mm Hg. Respirations are shallow with a rate of 50/minute. There is symmetric weakness of the face and all four extremities. Deep tendon reflexes are absent. Sensation is intact. What is the most likely diagnosis?
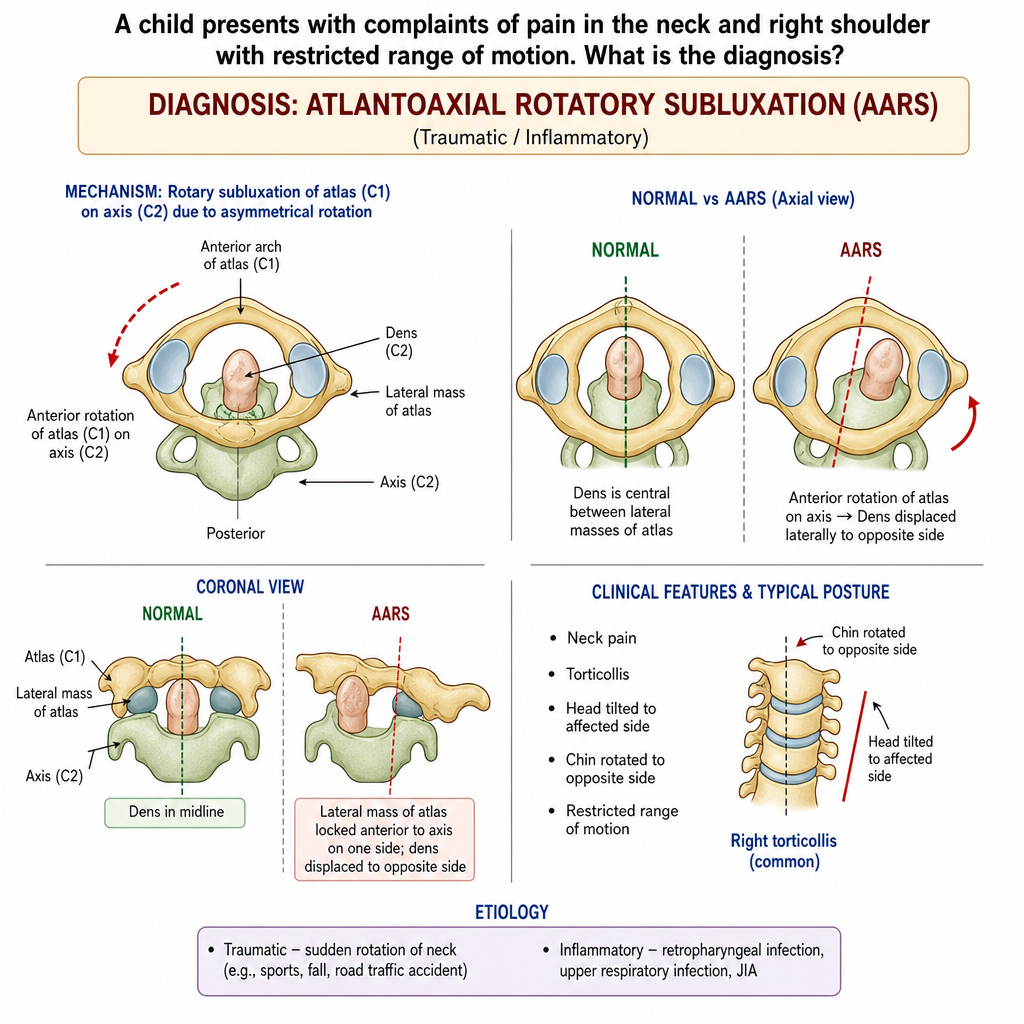
A child presents with acute onset of neck pain and right shoulder pain with restricted range of motion. He had a minor fall 2 days ago. On examination, the head is tilted to one side with the chin rotated to the opposite side. What is the diagnosis?
What is true about the severity of limb affection in Spastic Diplegia of Cerebral Palsy?
What is the most frequent form of childhood epilepsy?
What is the diagnosis in an infant presenting with a large head?
A six-month-old baby girl, who was normal at birth, begins to show signs of motor retardation. While she could sit up at 5 months, she can no longer do so. As time goes on, the child continues to deteriorate and eventually becomes unresponsive to visual or auditory stimuli. Funduscopic examination reveals cherry-red macular spots in both eyes. Which of the following genetic abnormalities is most often related to the development of this disease?
A 6-month-old child presents with port wine stain, mental retardation, and recurrent focal seizures. Which of the following is NOT true about the condition?
Pseudohypertrophy of muscles is seen in which of the following conditions?
A 6-year-old child presents with acute onset of fever (104°F) and febrile seizures. What prophylactic measure should be recommended to prevent future recurrence of seizures?
Practice by Chapter
Seizure Disorders and Epilepsy
Practice Questions
Febrile Seizures
Practice Questions
Headache Disorders
Practice Questions
Cerebral Palsy
Practice Questions
Neural Tube Defects
Practice Questions
Neuromuscular Disorders
Practice Questions
Neurodegenerative Disorders
Practice Questions
CNS Infections
Practice Questions
Hydrocephalus
Practice Questions
Movement Disorders
Practice Questions
Traumatic Brain Injury
Practice Questions
Neuroimaging in Pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app