
Neurology — MCQs

On this page
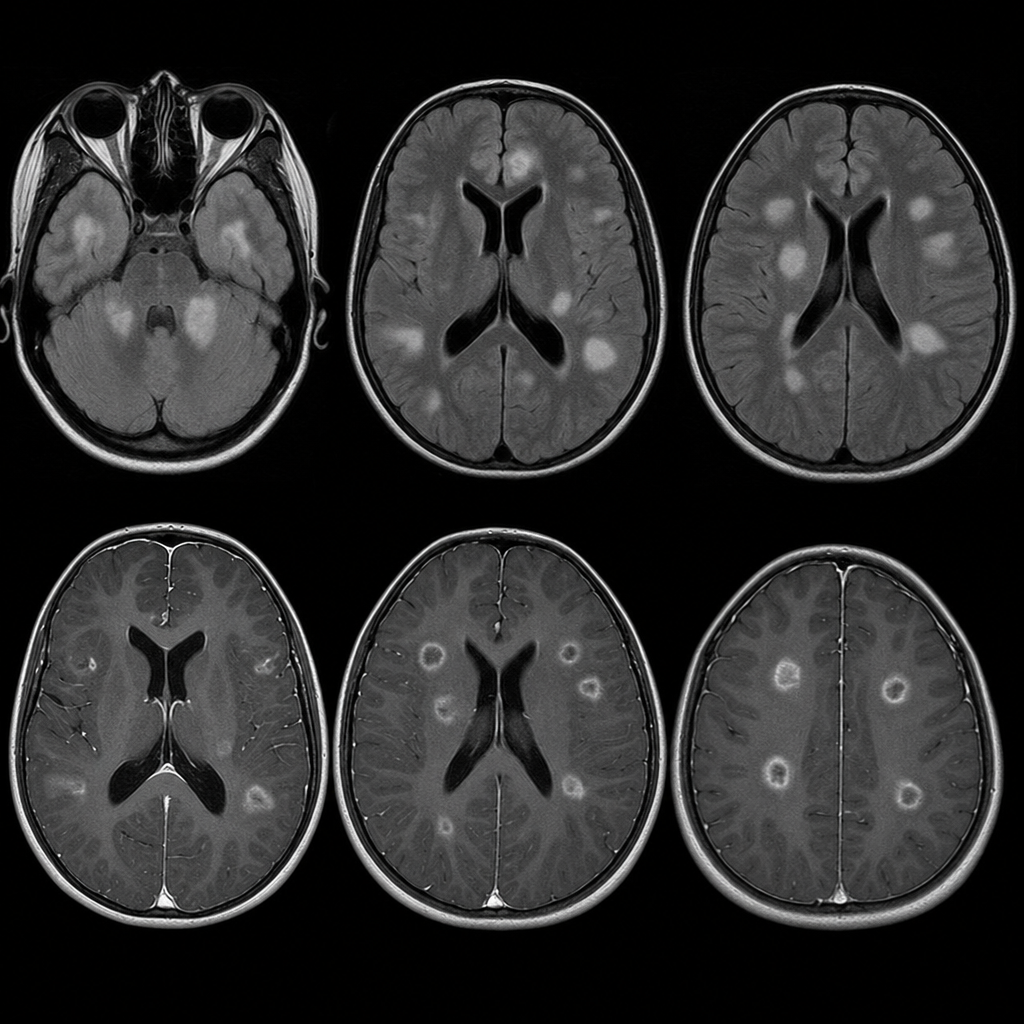
The 7-year-old boy, who is now in your office, was last seen 2 weeks ago with a mild viral upper respiratory tract infection. However, he presents today with fever, ataxia, weakness, headache, vomiting, and confusion with altered behavior that is out of proportion to his fever. In the office, he experiences a 3-minute left-sided tonic-clonic seizure. After sending him to the hospital and ordering a magnetic resonance imaging (MRI) with contrast of the brain, the results of which are shown, his likely diagnosis is which of the following?
The following are recognized signs and symptoms of raised intracranial tension in a 9-month-old infant, except which of the following?
Which of the following is the most common cause of a bulging anterior fontanelle in infants?
Which of the following is a symptom of cerebral palsy?
Febrile seizures occur most frequently in children of which age group?
The drug of choice for infantile spasms in a patient with tuberous sclerosis is:
What is the first-line treatment for West syndrome in a child with Tuberous Sclerosis?
Practice by Chapter
Seizure Disorders and Epilepsy
Practice Questions
Febrile Seizures
Practice Questions
Headache Disorders
Practice Questions
Cerebral Palsy
Practice Questions
Neural Tube Defects
Practice Questions
Neuromuscular Disorders
Practice Questions
Neurodegenerative Disorders
Practice Questions
CNS Infections
Practice Questions
Hydrocephalus
Practice Questions
Movement Disorders
Practice Questions
Traumatic Brain Injury
Practice Questions
Neuroimaging in Pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app