
Neurology — MCQs

On this page
What is the typical maintenance dose of Levetiracetam in pediatric patients?
A 1-day-old male baby delivered by LSCS presents with swelling over the back in the midline. What is the most likely diagnosis?
What is the recurrence rate of febrile seizures?
A 10-month-old infant was brought with complaints of jerking movements of limbs towards the body. On examination, there is regression of developmental milestones. Electroencephalogram shows hypsarrhythmia. What is the most appropriate first-line treatment?
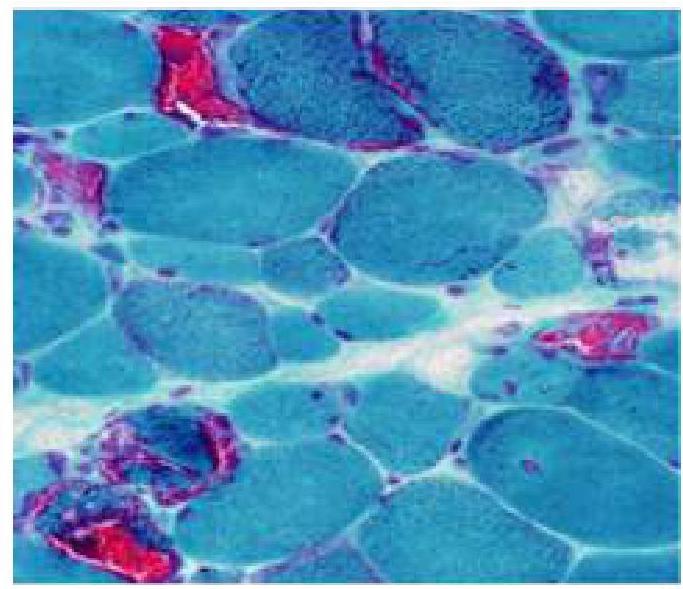
An 8-year old child has difficulty walking and getting up from a squatting position. A muscle biopsy was done and is as shown in the image. Which of the following is true about this condition?
Which of the following is not a known cause of neuroregression in children?
What is the preferred medication for treating severe cases of rheumatic chorea that do not respond to standard treatments?
Which of the following statements about encephalocoele is false?
A young child presents with episodes of inappropriate laughter. What is the most likely diagnosis?
What is the significance of the persistence of the asymmetric tonic neck reflex in a 9-month-old infant?
Practice by Chapter
Seizure Disorders and Epilepsy
Practice Questions
Febrile Seizures
Practice Questions
Headache Disorders
Practice Questions
Cerebral Palsy
Practice Questions
Neural Tube Defects
Practice Questions
Neuromuscular Disorders
Practice Questions
Neurodegenerative Disorders
Practice Questions
CNS Infections
Practice Questions
Hydrocephalus
Practice Questions
Movement Disorders
Practice Questions
Traumatic Brain Injury
Practice Questions
Neuroimaging in Pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app