
Neurology — MCQs

On this page
First-line acute management of febrile convulsion in hospital setting includes
A mother brought her child who has got a vascular plaque like lesion over the lateral aspect of forehead mainly involving ophthalmic and maxillary division of trigeminal nerve. Mother says that the lesion has remained unchanged since birth. Also mother gives a history that the child is on valproate for seizure disorder. What is the MOST probable diagnosis?
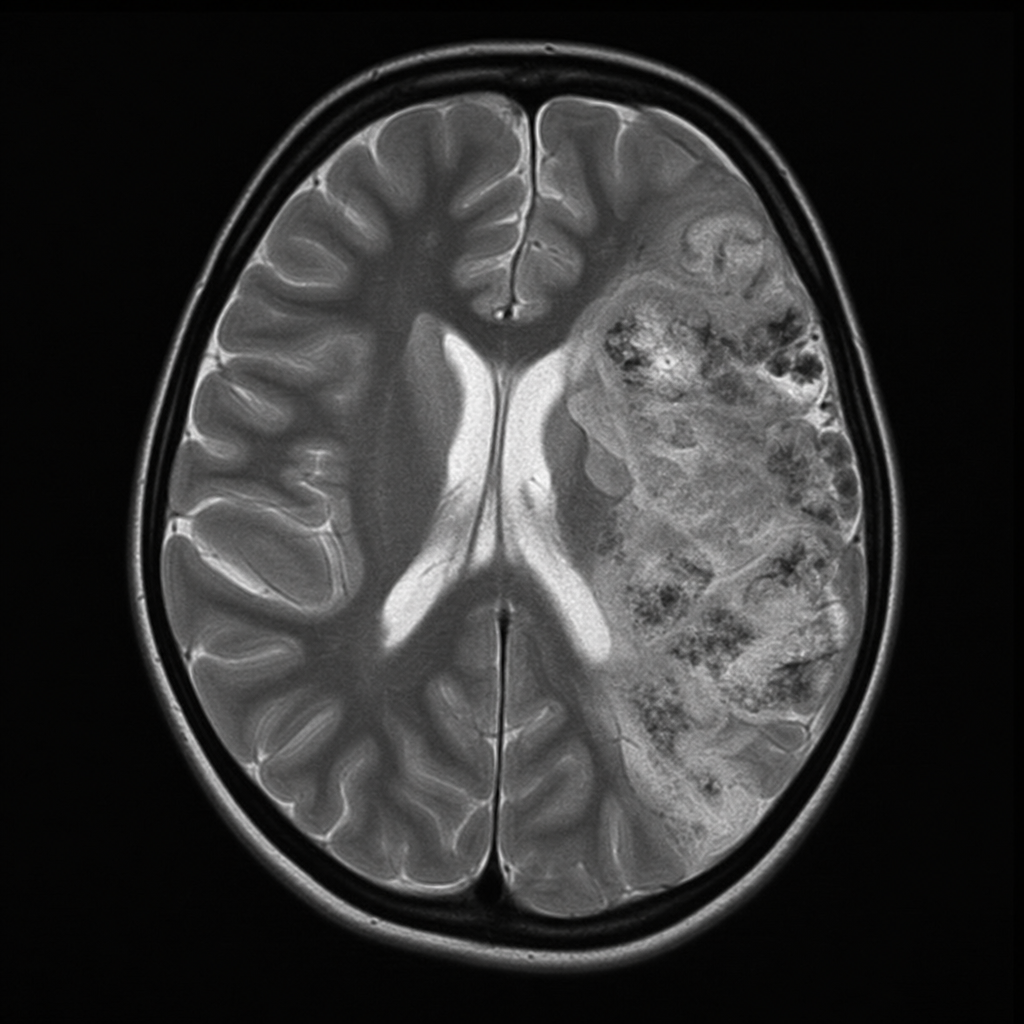
MRI scan of a child with intellectual disability, recurrent seizures and facial port-wine capillary malformation in the trigeminal distribution. Diagnosis is?
Child was seen taking off clothes while watching TV; he suddenly closed eyes for some time and was lethargic after some time. He had probably
Give the most probable diagnosis of a 1 yr. old child of normal intelligence with features of hypotonia. On examination there are tongue fasciculations and he keeps his body in a frog like position ?
A 9 year old female patient has come for routine dental examination. She is unable to articulate her words properly. General examination reveals muscle weakness and stiffness, irregular gait, uncoordinated and involuntary movements, chewing and swallowing difficulties as well as speech problems. Which of the following may not be an etiologic factor for this condition?
A 9 year old female patient has come for a routine dental examination. She is unable to articulate her words properly. General examination reveals muscle weakness and stiffness, irregular gait, uncoordinated and involuntary movements, chewing and swallowing difficulties as well as speech problems. Which of the following reflexes maybe absent in this patient?
Febrile seizure persisting continuously beyond ____ should be treated with midazolam nasal spray:
Which of the following is true about febrile convulsions?
A 7-year old boy presents with a right-sided hemangioma and left-sided focal seizures. The most likely diagnosis is:
Practice by Chapter
Seizure Disorders and Epilepsy
Practice Questions
Febrile Seizures
Practice Questions
Headache Disorders
Practice Questions
Cerebral Palsy
Practice Questions
Neural Tube Defects
Practice Questions
Neuromuscular Disorders
Practice Questions
Neurodegenerative Disorders
Practice Questions
CNS Infections
Practice Questions
Hydrocephalus
Practice Questions
Movement Disorders
Practice Questions
Traumatic Brain Injury
Practice Questions
Neuroimaging in Pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app