
Neurology — MCQs

On this page
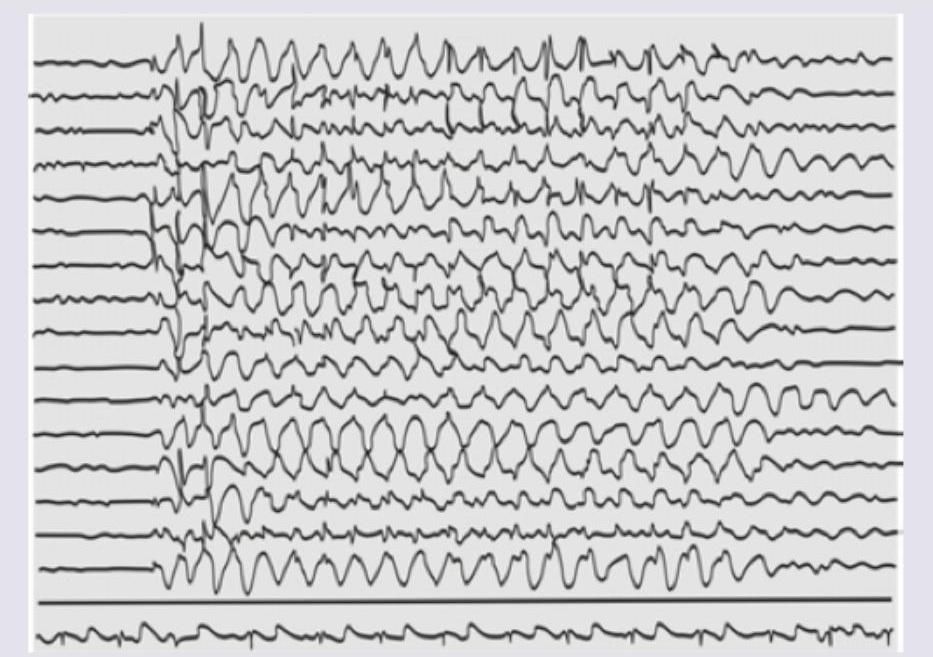
A 7-year-old girl is easily distracted in class and exhibits poor scholastic performance. The EEG is shown. What is the most likely diagnosis? (AIIMS May 2014)
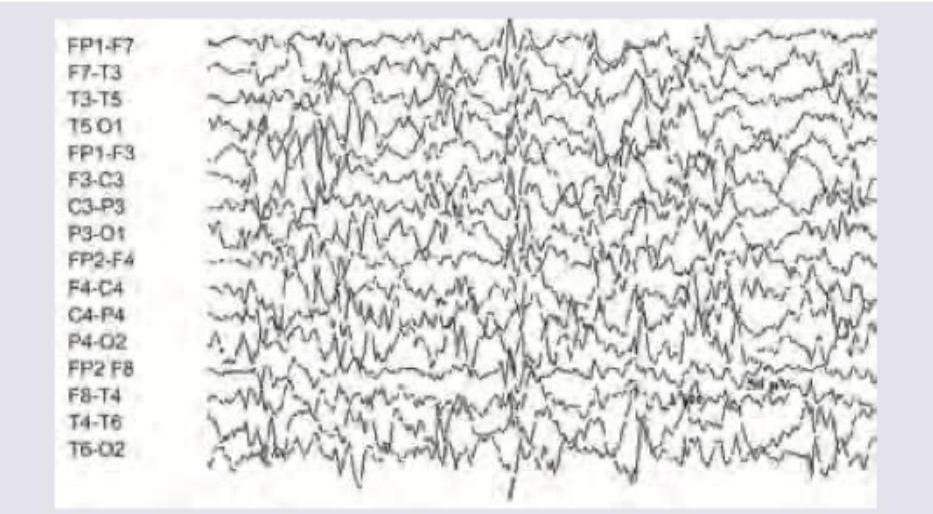
The EEG of an infant with early morning jerks shows?
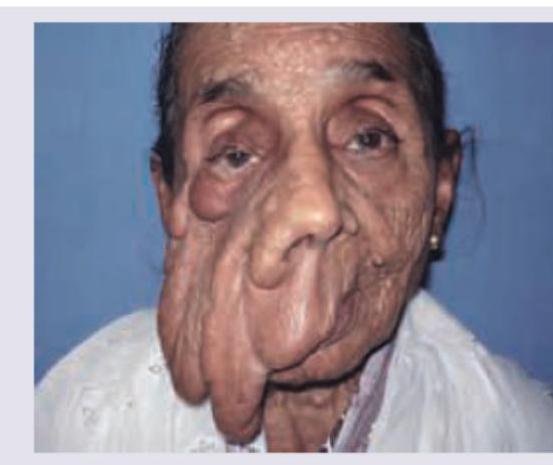
Comment on the diagnosis based on the image shown below. (Recent NEET Pattern 2016-17)
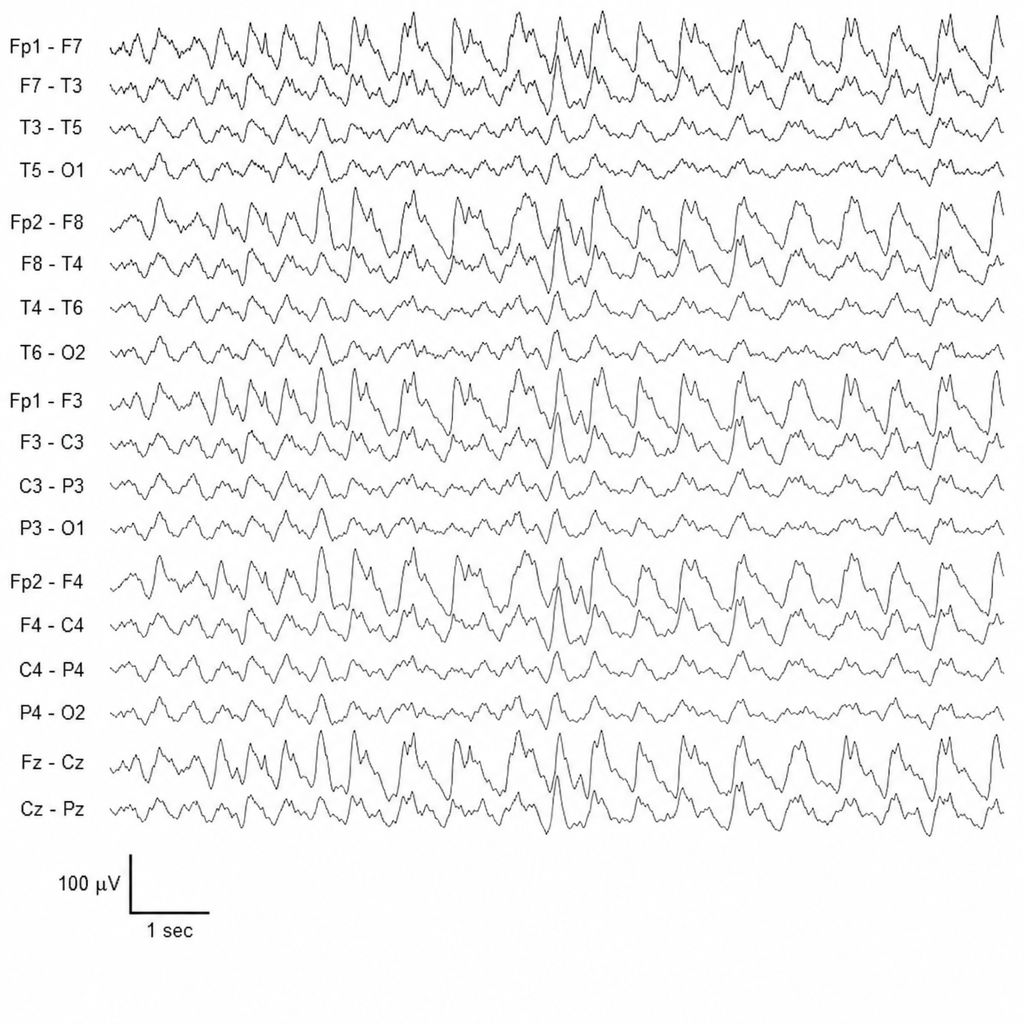
A 1-year-old child presents with infantile spasms. EEG done shows: (Recent NEET Pattern 2016-17)
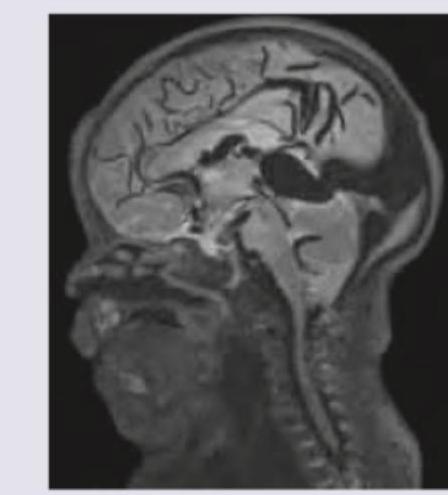
A 6 month infant was brought with complaints of a failure to gain weight and a large head. On examination, increased head circumference, bounding pulses and features of heart failure were noted. On cranial auscultation loud cranial bruit was heard. MRI head shows? (Recent NEET Pattern 2018-19)
Which of the following are tools commonly used in the evaluation of children with cerebral palsy for motor function and spasticity assessment? I. Gross Motor Function Classification System II. Medical Research Council System III. Modified Connors Scale (Connors-II) IV. Modified Ashworth Scale Select the correct answer using the code given below:
Which of the following are characteristic features of cerebral palsy? I. Disorder of movement II. Permanent nature III. Progressive course IV. Disorder of posture Select the correct answer using the code given below :
Which one of the following childhood epileptic disorders often needs long term treatment with antiepileptic drugs?
Neural tube defects have which one of the following inheritance patterns ?
The congenital abnormality which is invariably lethal is:
Practice by Chapter
Seizure Disorders and Epilepsy
Practice Questions
Febrile Seizures
Practice Questions
Headache Disorders
Practice Questions
Cerebral Palsy
Practice Questions
Neural Tube Defects
Practice Questions
Neuromuscular Disorders
Practice Questions
Neurodegenerative Disorders
Practice Questions
CNS Infections
Practice Questions
Hydrocephalus
Practice Questions
Movement Disorders
Practice Questions
Traumatic Brain Injury
Practice Questions
Neuroimaging in Pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app