
Neurology — MCQs

On this page
A 3-year-old child is brought to the emergency room with a generalized seizure following a high-grade fever. What is the first-line drug of choice for seizure control in this acute febrile setting?
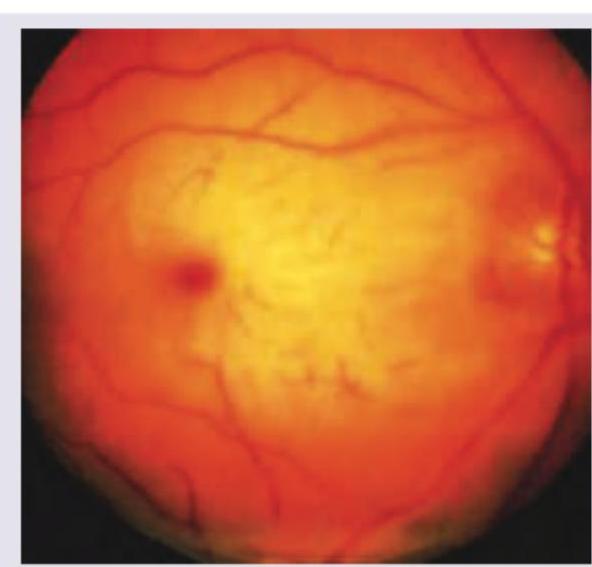
A child presents with regression of milestones and has become blind. On examination spasticity is noted in both legs. Fundus examination reveals a cherry-red spot at the macula with surrounding retinal whitening. Which category of brain tissue degeneration does this disorder represent? (Recent NEET Pattern 2016-17)
The following medical condition is associated with all except:

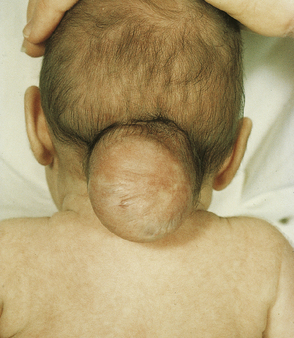
Identify the congenital defect seen in this baby.
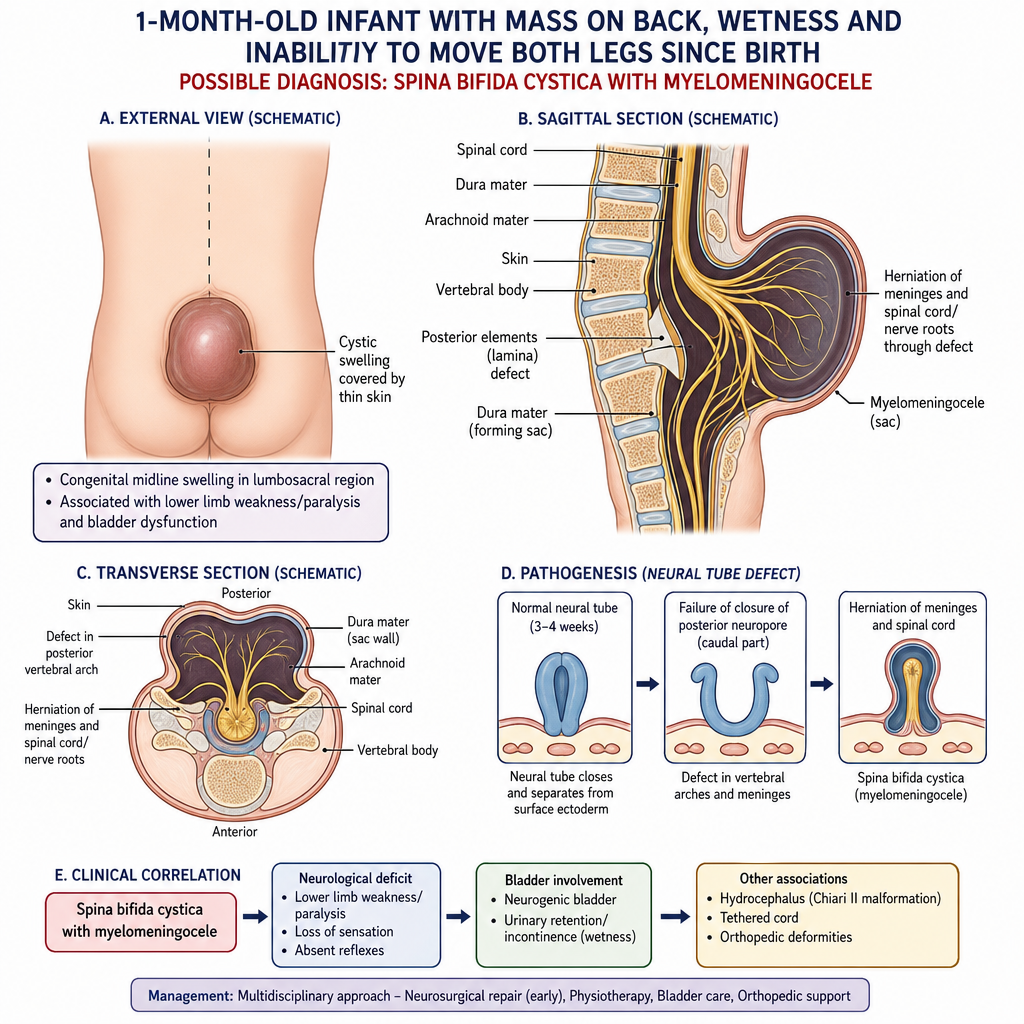
A 1-month-old baby brought by the mother complaining of a mass on back associated with CSF leakage and inability of both legs to move ever since birth. Possible diagnosis: (Recent NEET Pattern 2016-17)
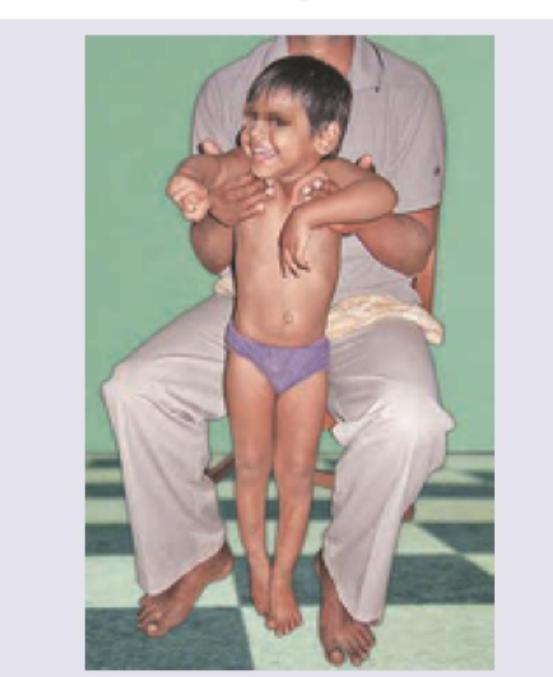
A child is having difficulty standing up from a sitting position and uses a characteristic maneuver shown in the image below. What is the most likely diagnosis?
Identify the following congenital defect. MRI confirms the presence of a neural placode (spinal cord tissue) within the sac:

CT scan of a child with intellectual disability, recurrent seizures and facial port-wine capillary malformation. Diagnosis is:
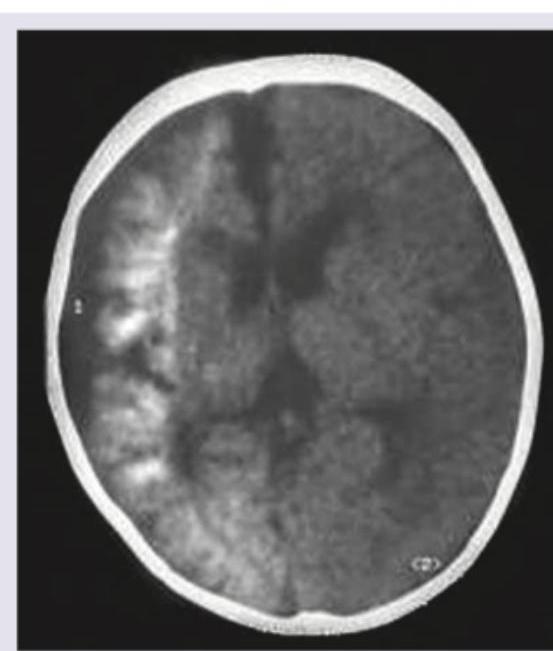
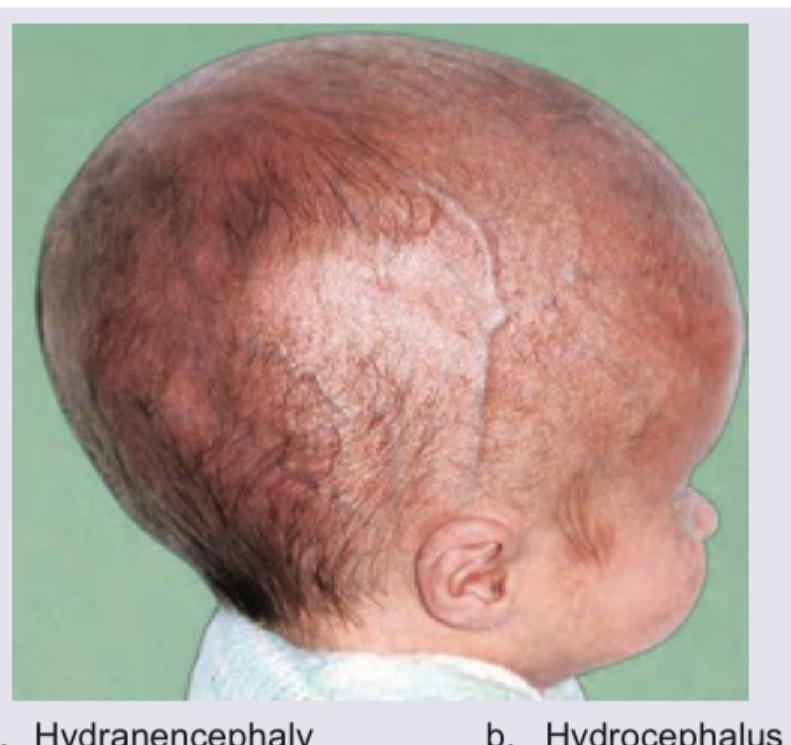
Comment on the diagnosis in this 1-year-old child:
Which finding is not associated with Sturge-Weber syndrome?

Practice by Chapter
Seizure Disorders and Epilepsy
Practice Questions
Febrile Seizures
Practice Questions
Headache Disorders
Practice Questions
Cerebral Palsy
Practice Questions
Neural Tube Defects
Practice Questions
Neuromuscular Disorders
Practice Questions
Neurodegenerative Disorders
Practice Questions
CNS Infections
Practice Questions
Hydrocephalus
Practice Questions
Movement Disorders
Practice Questions
Traumatic Brain Injury
Practice Questions
Neuroimaging in Pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app