
Neurology — MCQs

On this page
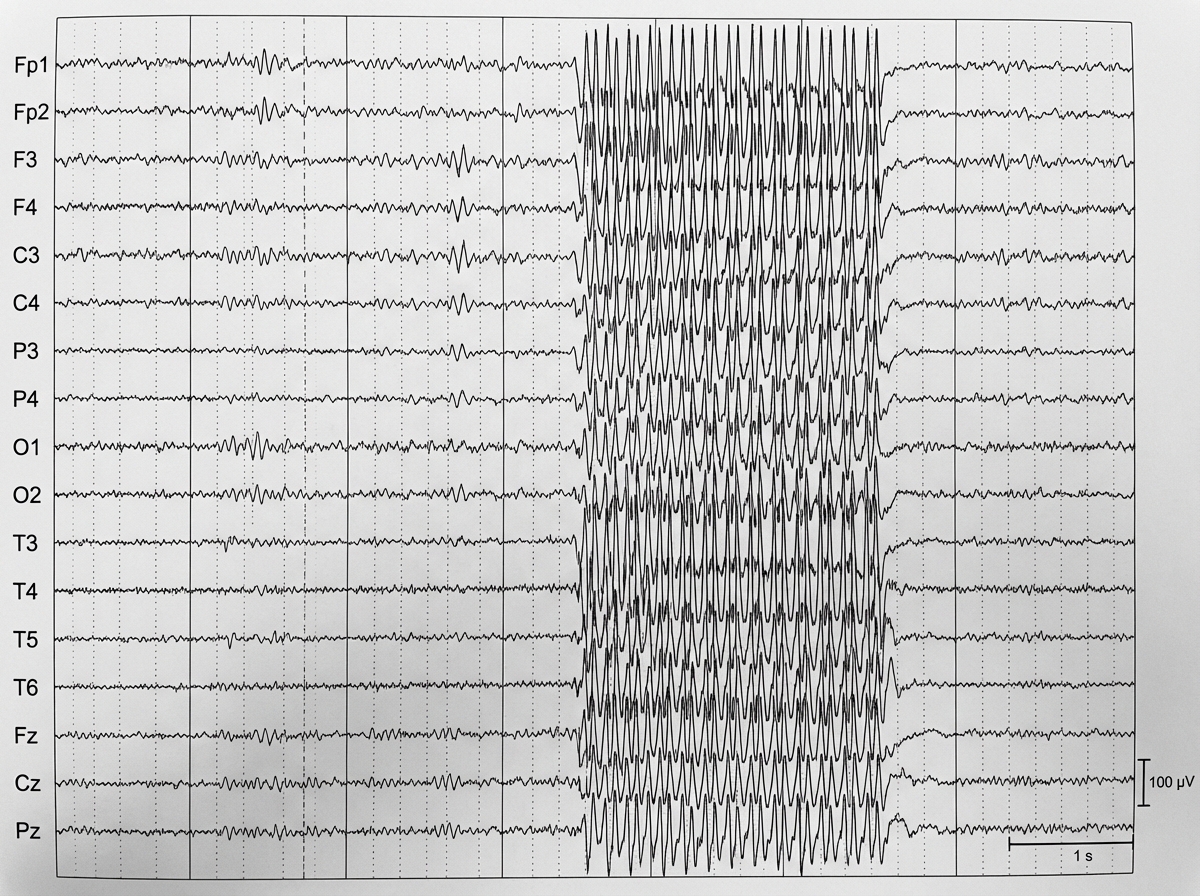
A 7-year-old boy, who gets easily distracted in class with poor academic performance, experiences a seizure episode after hyperventilation. What is the diagnosis suggested by the EEG findings shown in the image?
A 10-year-old girl develops ataxia and hydrocephalus. A CT scan shows a midline cerebellar mass. Which of the following is the most likely diagnosis?
What is the most common age group for febrile seizures?
Which of the following is NOT true about Duchenne Muscular Dystrophy?
Which of the following statements about Duchenne muscular dystrophy is false?
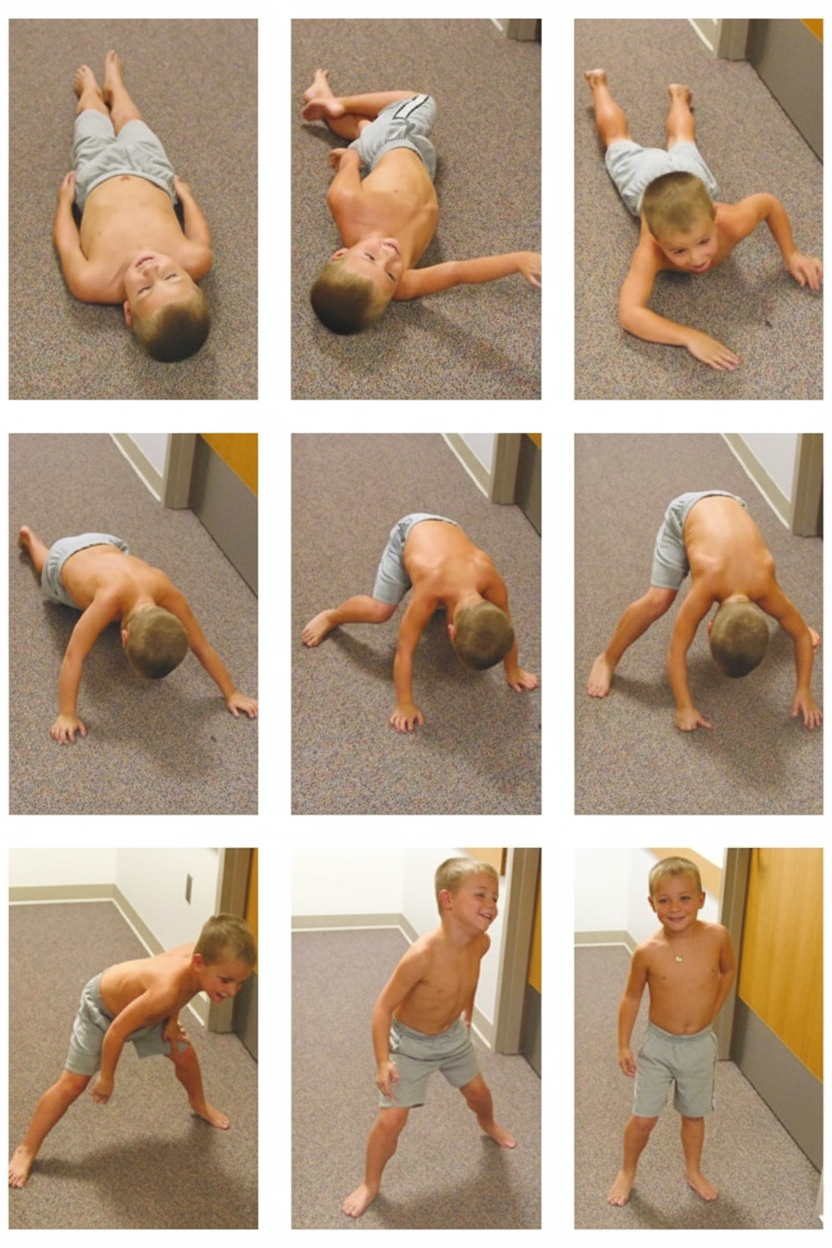
An 8-year-old boy presents with progressive difficulty in walking since age 4, pseudohypertrophy of the calf muscles, and a markedly elevated CK. What is the most likely diagnosis?
What is the commonest cause of non-communicating hydrocephalus in children?
The 'sunset sign' is observed in which of the following conditions?
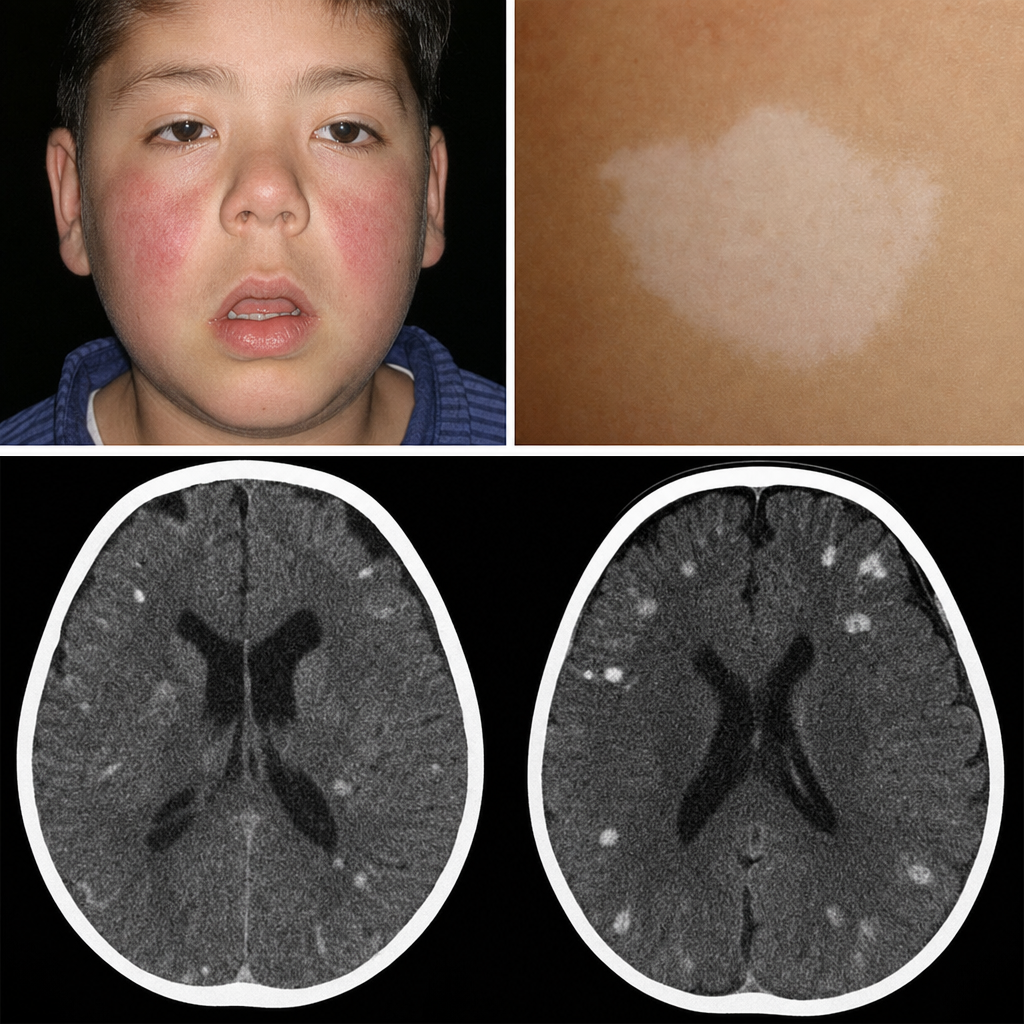
A child with mental retardation and multiple reddish-brown papules over the nasolabial folds and cheeks (facial angiofibromas) undergoes a CT scan. What is the most likely diagnosis?
Hung up reflex is seen in?
Practice by Chapter
Seizure Disorders and Epilepsy
Practice Questions
Febrile Seizures
Practice Questions
Headache Disorders
Practice Questions
Cerebral Palsy
Practice Questions
Neural Tube Defects
Practice Questions
Neuromuscular Disorders
Practice Questions
Neurodegenerative Disorders
Practice Questions
CNS Infections
Practice Questions
Hydrocephalus
Practice Questions
Movement Disorders
Practice Questions
Traumatic Brain Injury
Practice Questions
Neuroimaging in Pediatrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app