
Neoplasia — MCQs

On this page
Which syndrome is associated with an inherited mutation of the p53 tumor suppressor gene?
Paraneoplastic syndrome Hypercalcemia of malignancy is produced due to ectopic production of which hormone by solid tumors like squamous cell carcinoma?
Grade of tumor denotes
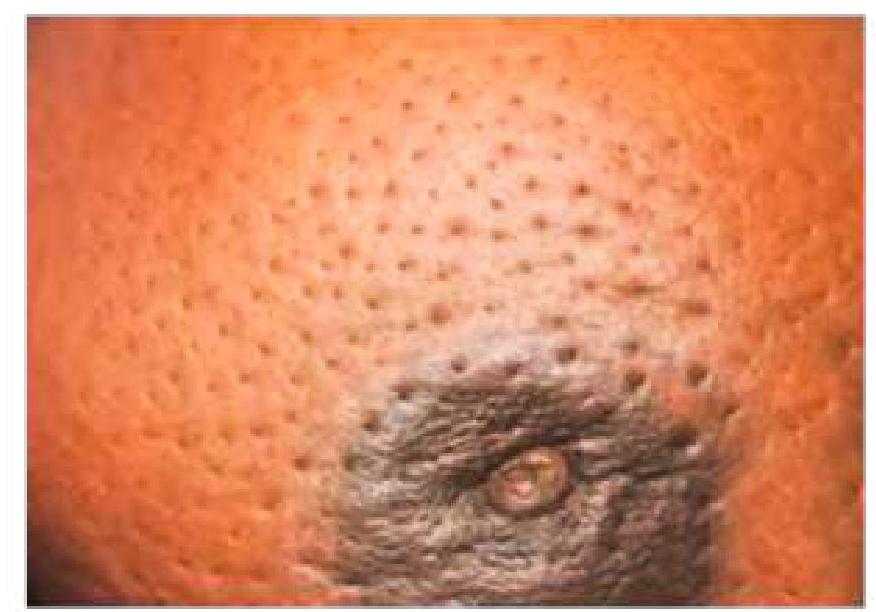
A 59-year-old lady presents with a progressive, painless lump in the breast. What is the cause of the skin change associated with breast cancer?
An elderly male is known as a smoker presented with chronic cough, significant weight loss, and fatigue. Serum calcium level is raised. A lung biopsy was done, and it showed large atypical cells with hyperchromasia. What is the probable diagnosis?
What is the T stage classification for a lung carcinoma measuring 2.5 cm and not involving the pleura?
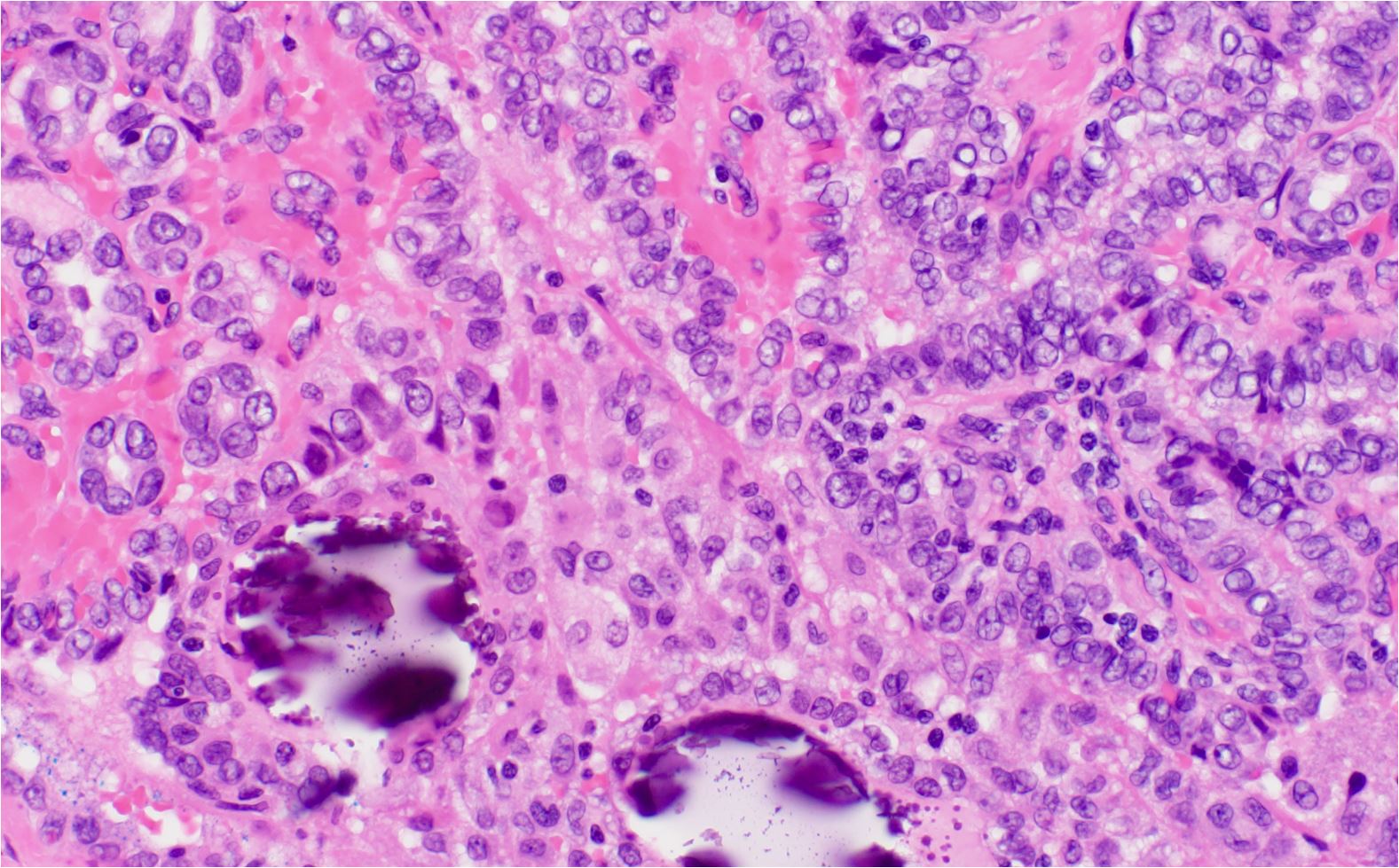
A 25-year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis based on the histological findings?
RET proto-oncogene is associated with the development of
Anaplasia is
Which is the most common type of male breast cancer?
Practice by Chapter
Nomenclature and Classification of Tumors
Practice Questions
Characteristics of Benign and Malignant Neoplasms
Practice Questions
Molecular Basis of Cancer
Practice Questions
Carcinogenesis and Carcinogens
Practice Questions
Tumor Progression and Metastasis
Practice Questions
Tumor Markers
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Genetic Basis of Cancer
Practice Questions
Tumor Immunity
Practice Questions
Cancer Epidemiology and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app