
Neoplasia — MCQs

On this page
All of the following constitute familial cancer syndromes except?
Which of the following is HMB45 negative?
All of the following are tumor suppressor genes except?
Which chromosome is associated with retinoblastoma?
Familial tendency is not seen in which of the following malignancies?
What is the most common sarcoma in a person receiving immunosuppressive treatment?
Which of the following statements about chromothrypsis is NOT true?
A woman who is heterozygous for glucose-6-phosphate dehydrogenase (G6PD), a polymorphic enzyme transcribed from the X chromosome, develops chronic myeloid leukemia. Restriction fragment length polymorphism (RFLP) studies on the tumor cells for G6PD reveal that only a single form of the enzyme is transcribed. This finding supports which of the following features of neoplasia?
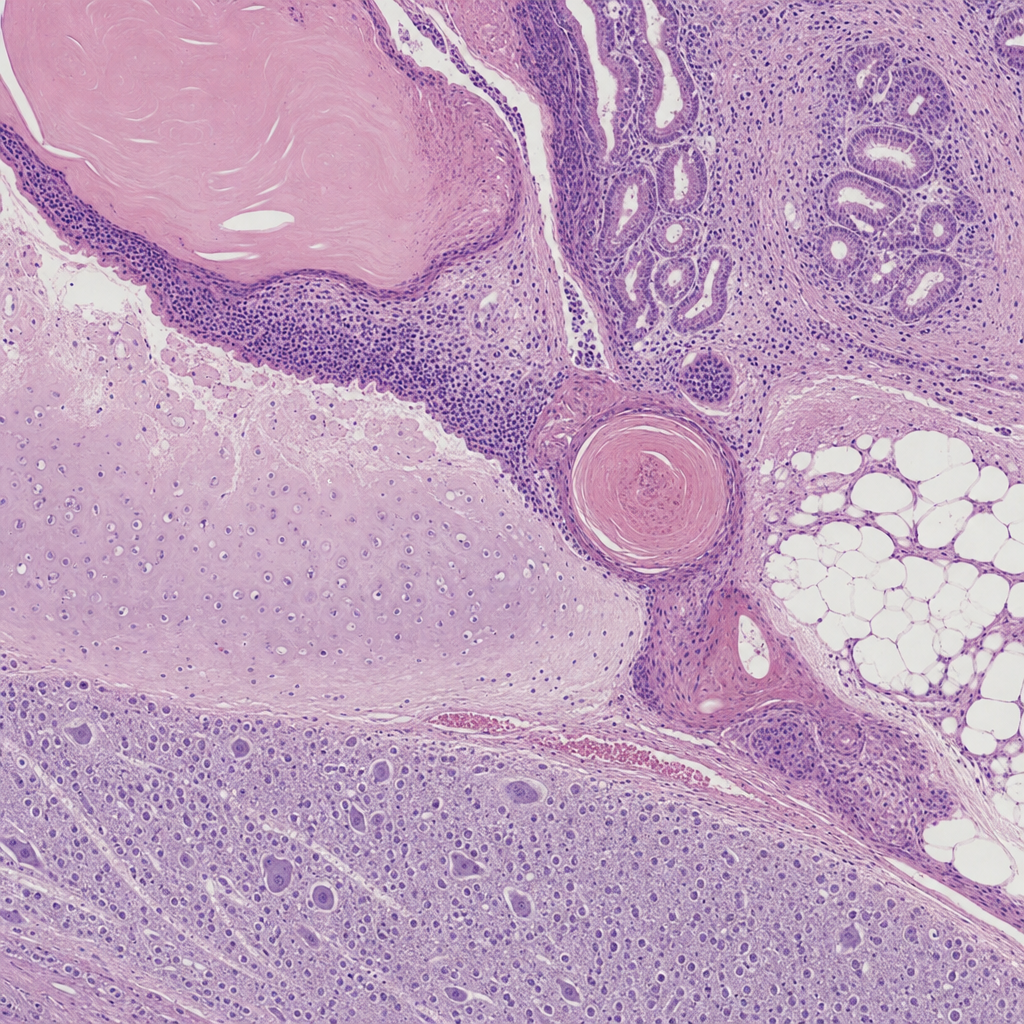
Comment on the histopathological specimen?
Malignancy is typically associated with disordered differentiation and mutation. Which of the following options best describes anaplasia?
Practice by Chapter
Nomenclature and Classification of Tumors
Practice Questions
Characteristics of Benign and Malignant Neoplasms
Practice Questions
Molecular Basis of Cancer
Practice Questions
Carcinogenesis and Carcinogens
Practice Questions
Tumor Progression and Metastasis
Practice Questions
Tumor Markers
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Genetic Basis of Cancer
Practice Questions
Tumor Immunity
Practice Questions
Cancer Epidemiology and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app