
Neoplasia — MCQs

On this page
All of the following are major subtypes of breast cancer based on Gene array analysis EXCEPT:
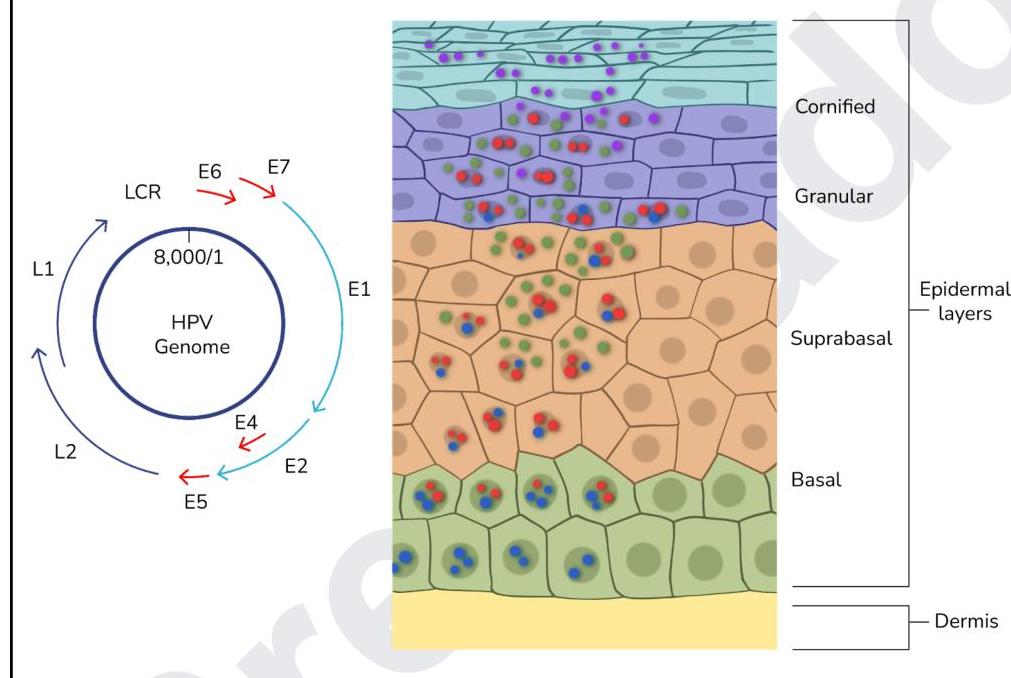
How do high-risk HPV types contribute to cervical carcinogenesis?
A patient has a cerebellar mass, renal tumor, and a family history of similar conditions. Which of the following mutations is most likely present in the family?
TTF-1 is a tumor marker for which of the following?
A 49 year old female presents with a breast lump. Which of the following findings is in accordance with basal-like breast cancer?
The image below shows the life cycle of a virus. Which of the proteins of the virus act as oncogenes?
Which of the following conditions is associated with perineural invasion?
What is the correct statement about thymoma?
Which of the following is an Anti-apoptotic gene?
A 32-year-old HIV-positive man presents with multiple flesh-colored, pedunculated lesions on his penis. Biopsy shows koilocytes and increased mitotic figures. Which of the following viral proteins is responsible for the cellular changes observed?
Practice by Chapter
Nomenclature and Classification of Tumors
Practice Questions
Characteristics of Benign and Malignant Neoplasms
Practice Questions
Molecular Basis of Cancer
Practice Questions
Carcinogenesis and Carcinogens
Practice Questions
Tumor Progression and Metastasis
Practice Questions
Tumor Markers
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Genetic Basis of Cancer
Practice Questions
Tumor Immunity
Practice Questions
Cancer Epidemiology and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app