
Neoplasia — MCQs

On this page
The malignancy associated with Stewart-Treves syndrome is
Which one of the following is NOT associated with BRCA1/BRCA2 genes?
In which of the following is the term low and high grade squamous intraepithelial neoplasia used?
Which one of the following is not an epithelial tumour of the ovary?
Which of the following pairs is not correctly matched?
Presence of signet-ring cells in a cellular or myxomatous stroma is diagnostic of:
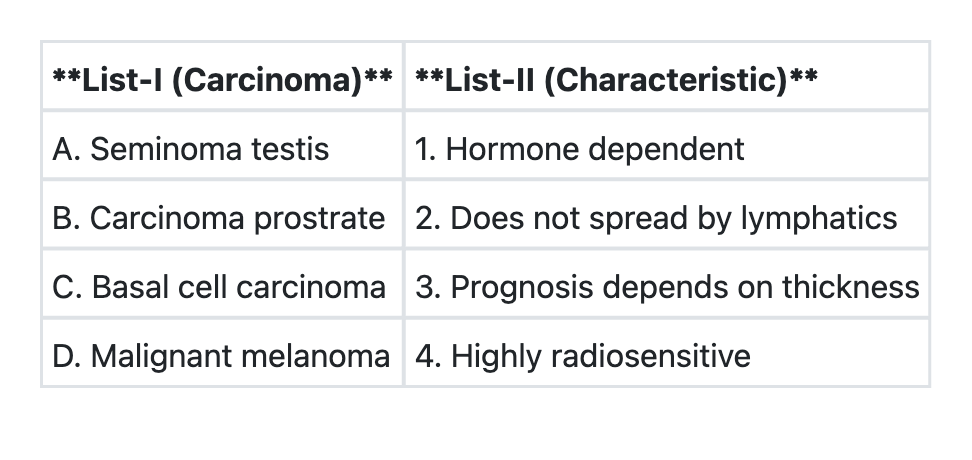
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which of the following statements regarding Paget's disease of nipple are correct? 1. It represents benign pathology of nipple areola complex 2. It is eczema like condition of nipple and areola 3. Erosion of nipple is seen 4. Nipple biopsy is required for definitive diagnosis Select the correct answer using the code given below:
No increased relative risk of invasive breast carcinoma based on histopathological examination of benign breast tissue is for all of the following EXCEPT:
Which of the statements regarding Salivary gland neoplasms are correct? 1. 80–90% of parotid tumors are benign 2. 90% of sublingual gland tumors are malignant 3. 60–70% of submandibular gland tumors are benign 4. Parotid gland is most common site for salivary gland tumors Select the correct answer using the code given below:
Practice by Chapter
Nomenclature and Classification of Tumors
Practice Questions
Characteristics of Benign and Malignant Neoplasms
Practice Questions
Molecular Basis of Cancer
Practice Questions
Carcinogenesis and Carcinogens
Practice Questions
Tumor Progression and Metastasis
Practice Questions
Tumor Markers
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Genetic Basis of Cancer
Practice Questions
Tumor Immunity
Practice Questions
Cancer Epidemiology and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app