
Neoplasia — MCQs

On this page
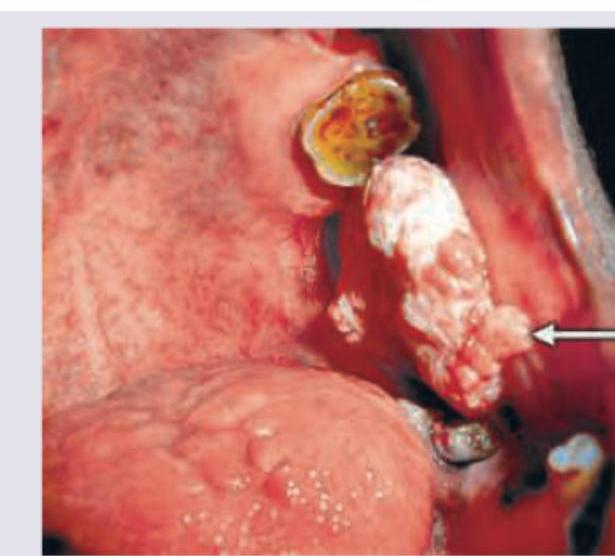
A patient presents with a gingival lesion as shown in the image. What is the most likely diagnosis?
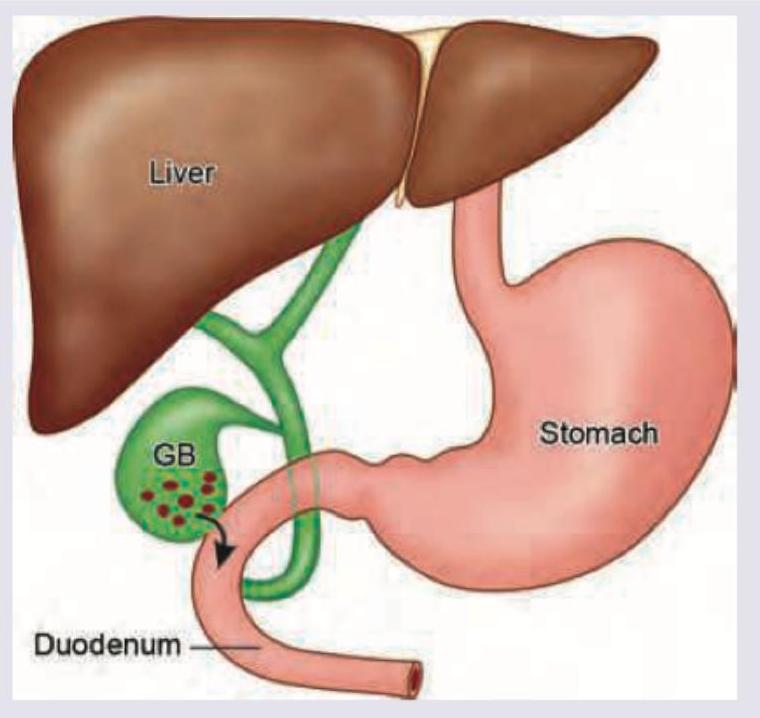
A patient with chronic cholelithiasis develops the complication shown in the image below. This leads to development of:
A 3-year-old child has presented with abdominal lump and peculiar appearance of eyes. All genes are responsible for development of this condition except:
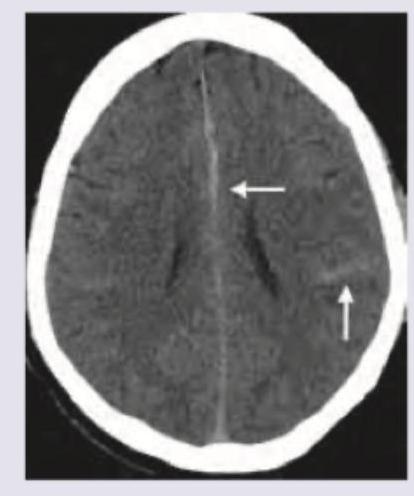
What is the correct diagnosis based on the image shown below?
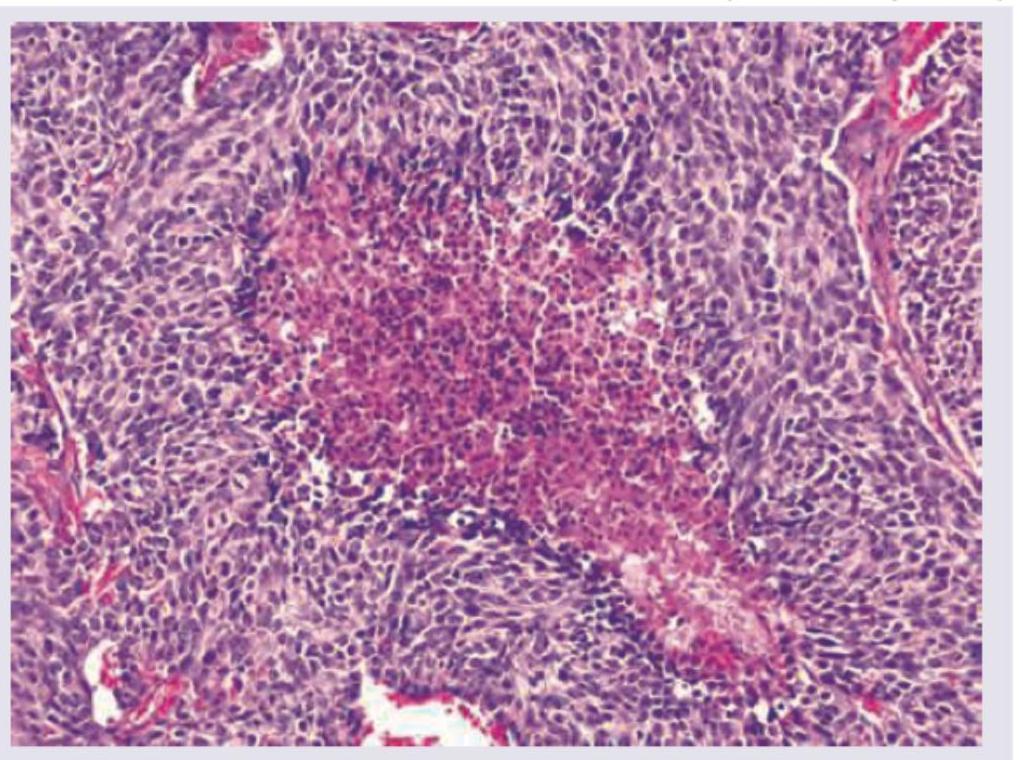
A 55-year-old male patient presented with a 4 month history of cough and hemoptysis. Bronchoscopy revealed an intrabronchial polyp. Biopsy from the polyp showed small cells with salt and pepper chromatin, with microscopic necrosis and 5 mitotic figures per 10 high power fields as shown below. Chromogranin staining was positive. What is the diagnosis and grade of the lesion?
Which of the following are poor prognostic factors in endometrial adenocarcinoma? I. Estrogen and progesterone receptor positivity II. HER-2/neu gene expression III. Histologic types papillary serous or clear cell carcinoma IV. Aneuploid tumours Select the correct answer using the code given below :
What is the most common type of tumour of Vermiform Appendix?
Which of the following are the malignancies associated with lymphoedema? I. Kaposi Sarcoma II. Squamous cell carcinoma III. Malignant melanoma IV. Leukaemia Select the correct answer using the code given below :
'Schiller-Duval body' is a characteristic histological feature of which one of the following cancers?
Masaoka staging is used for staging:
Practice by Chapter
Nomenclature and Classification of Tumors
Practice Questions
Characteristics of Benign and Malignant Neoplasms
Practice Questions
Molecular Basis of Cancer
Practice Questions
Carcinogenesis and Carcinogens
Practice Questions
Tumor Progression and Metastasis
Practice Questions
Tumor Markers
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Genetic Basis of Cancer
Practice Questions
Tumor Immunity
Practice Questions
Cancer Epidemiology and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app