
Neoplasia — MCQs

On this page
All of the following are major subtypes of breast cancer based on Gene array analysis EXCEPT:
A patient has a cerebellar mass, renal tumor, and a family history of similar conditions. Which of the following mutations is most likely present in the family?
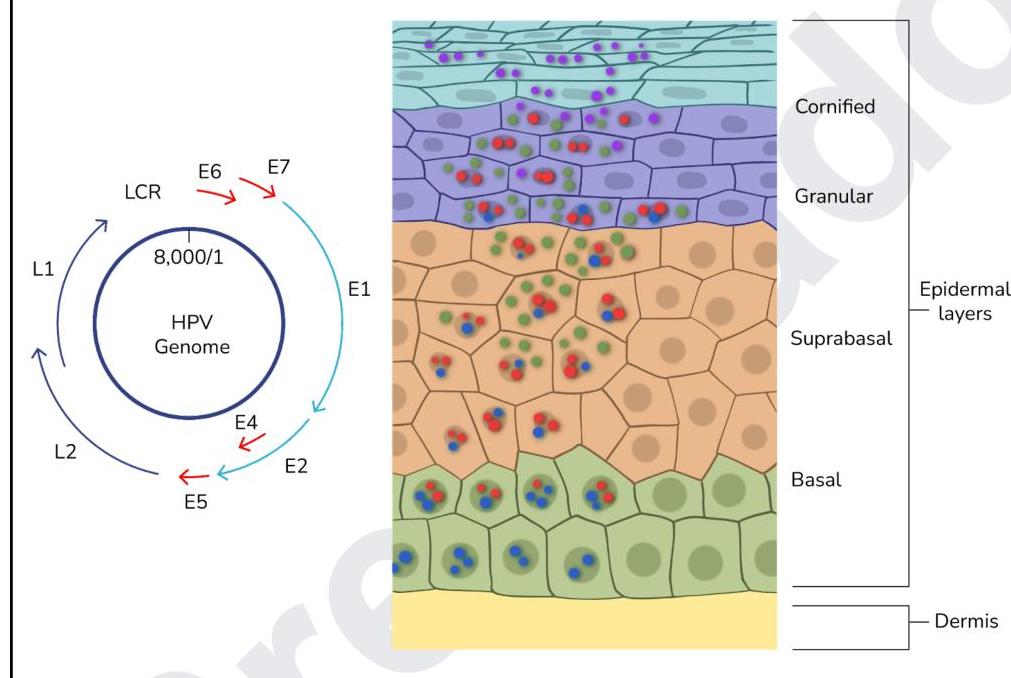
The image below shows the life cycle of a virus. Which of the proteins of the virus act as oncogenes?
Which of the following conditions is associated with perineural invasion?
What is the correct statement about thymoma?
Which of the following is NOT typically associated with chronic HPV infection?
A researcher is studying the ability of breast cancer cells to metastasize. Neoplastic cells obtained from 30 patients with stage IV ductal carcinoma of the breast are tagged with a fluorescent antibody. The cells are then inserted into a medium resembling normal human tissue. After 2 weeks, all samples show in vitro hematogenous invasion and migration away from the original site of insertion. Which of the following properties is most likely responsible for the ability of these neoplastic cells to metastasize?
A 70-year-old man comes to the physician because of a 4-month history of epigastric pain, nausea, and weakness. He has smoked one pack of cigarettes daily for 50 years and drinks one alcoholic beverage daily. He appears emaciated. He is 175 cm (5 ft 9 in) tall and weighs 47 kg (103 lb); BMI is 15 kg/m2. He is diagnosed with gastric cancer. Which of the following cytokines is the most likely direct cause of this patient’s examination findings?
Which of the following is true about Anaplasia?
Field carcinogenesis theory is commonly seen in
Practice by Chapter
Nomenclature and Classification of Tumors
Practice Questions
Characteristics of Benign and Malignant Neoplasms
Practice Questions
Molecular Basis of Cancer
Practice Questions
Carcinogenesis and Carcinogens
Practice Questions
Tumor Progression and Metastasis
Practice Questions
Tumor Markers
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Genetic Basis of Cancer
Practice Questions
Tumor Immunity
Practice Questions
Cancer Epidemiology and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app