
Dermatopathology — MCQs

On this page
HMB 45 is a tumor marker for which of the following neoplasms?
All of the following are premalignant lesions except:
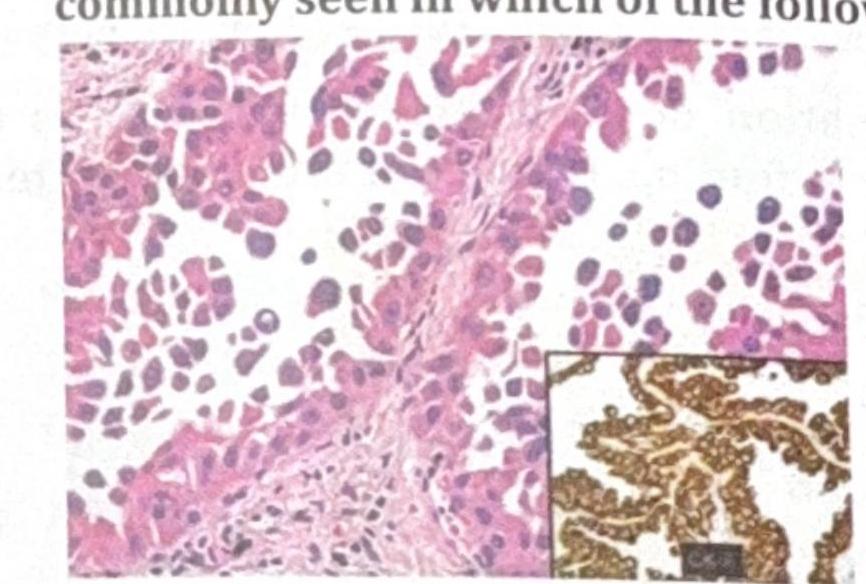
The skin biopsy shown below is most consistent with which of the following conditions? 
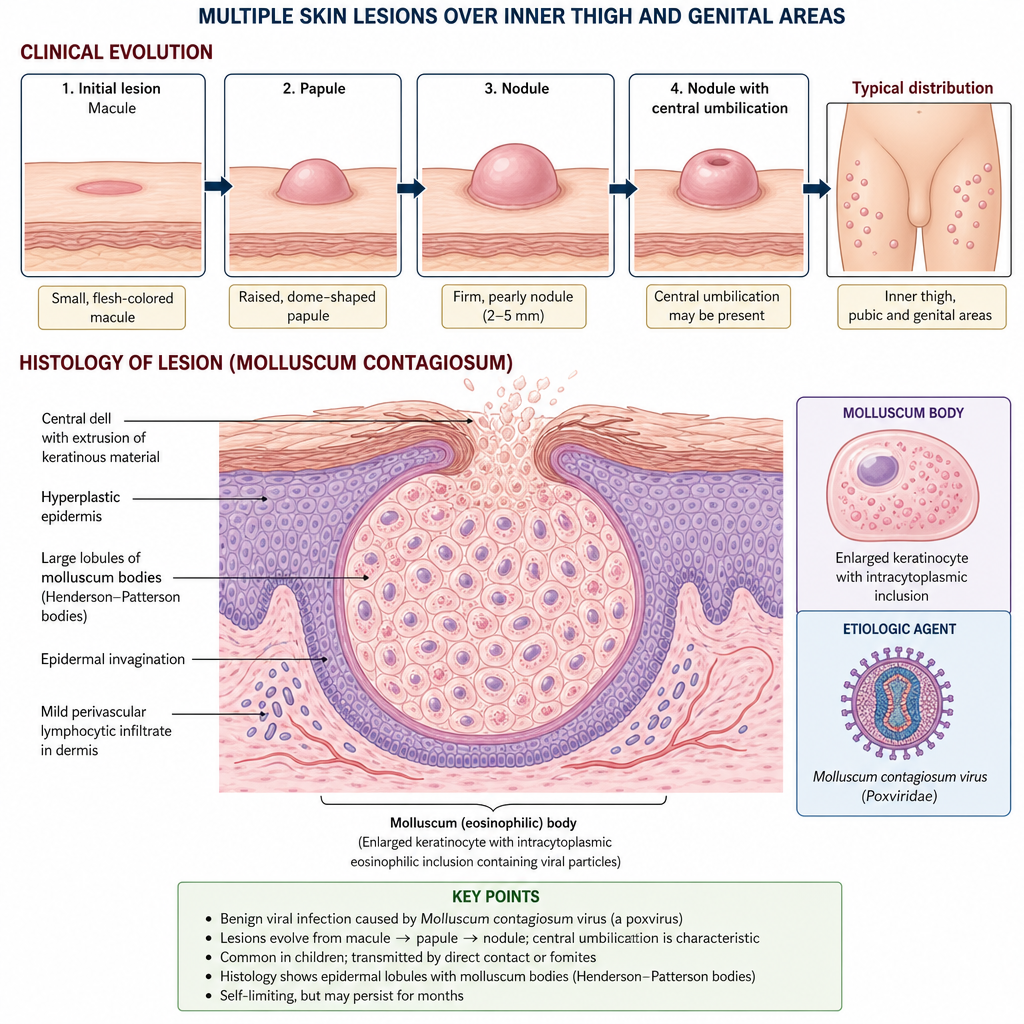
A child presents with multiple skin lesions over the inner thigh and genital areas. It initially started as macule and later developed to become nodules. Some nodules have central umbilication. The histology of the lesion is shown below
Which of the following structures is pathognomonic for chromoblastomycosis?
A skin biopsy shows 'snowstorm' appearance on polarized microscopy. Which histological finding would best confirm gouty tophi?
A skin biopsy shows 'tadpole' appearance of melanocytes. Which histological pattern would confirm Spitz nevus?
A skin biopsy shows 'crown of thorns' pattern on immunofluorescence. Which additional finding would confirm IgA vasculitis?
Munro's microabscesses are seen in all of the following except:
Parakeratosis is defined as:
Practice by Chapter
Structure and Function of Skin
Practice Questions
Inflammatory Dermatoses
Practice Questions
Blistering Diseases
Practice Questions
Infectious Diseases of the Skin
Practice Questions
Disorders of Pigmentation
Practice Questions
Benign Skin Tumors
Practice Questions
Malignant Skin Tumors
Practice Questions
Connective Tissue Disorders of the Skin
Practice Questions
Cutaneous Manifestations of Systemic Disease
Practice Questions
Hair and Nail Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app