
Dermatopathology — MCQs

On this page
What is the term for a swollen degenerating epithelial cell that results from acantholysis?
All of the following are markers of melanoma except?
Biopsy from a mole on the foot shows cytologic atypia of melanocytes and diffuse epidermal infiltration by anaplastic cells, which are also present in the papillary and reticular dermis. What is the most likely diagnosis?
Munro's microabscesses are typically seen in which layer of the epidermis?
Intraepithelial vacuolation with formation of a vesicle or bulla intraepithelially above the basal layer is characteristically seen in which of the following conditions?
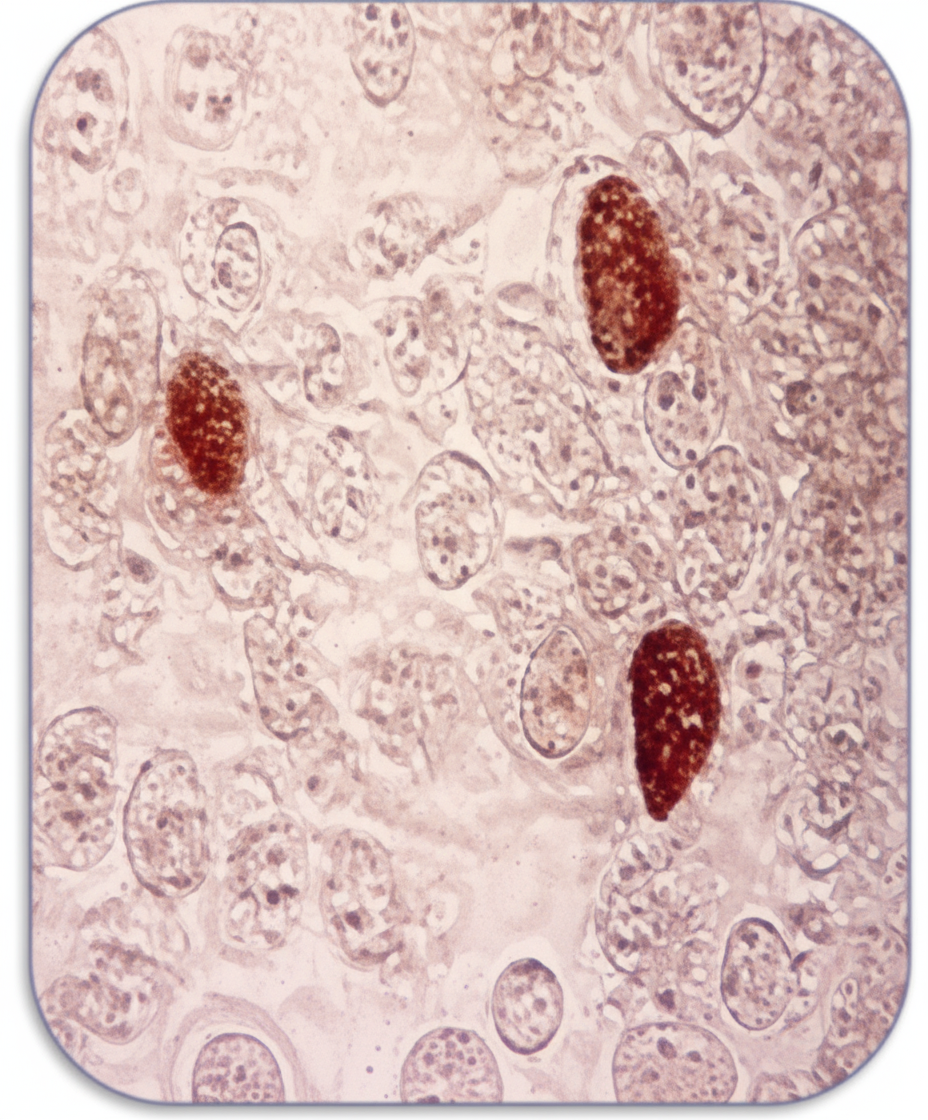
Histopathological diagram of a lesion shows characteristic intracytoplasmic viral inclusion bodies. Which virus is responsible for these inclusions?
"Church spire effect" is shown by which of the following conditions?
Which cancer is known to develop in chronic ulcers?
Examination of a skin lesion demonstrates very abnormal squamous cells with a high nuclear/cytoplasmic ratio and clumped chromatin. These cells form nests within the epidermis that extend to the superficial surface of the epithelium. In some places, nests of these cells have central areas of abnormal keratin formation. The basement membrane is intact and no nests of cells are seen in the dermis. Which of the following terms best describes this lesion?
Skin biopsy in leprosy is characterized by which of the following?
Practice by Chapter
Structure and Function of Skin
Practice Questions
Inflammatory Dermatoses
Practice Questions
Blistering Diseases
Practice Questions
Infectious Diseases of the Skin
Practice Questions
Disorders of Pigmentation
Practice Questions
Benign Skin Tumors
Practice Questions
Malignant Skin Tumors
Practice Questions
Connective Tissue Disorders of the Skin
Practice Questions
Cutaneous Manifestations of Systemic Disease
Practice Questions
Hair and Nail Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app