
Dermatopathology — MCQs

On this page
A 25-year-old woman develops extensive pruritic wheals following ingestion of seafood to which she was allergic. While these lesions are usually not biopsied, a biopsy would probably show which of the following features?
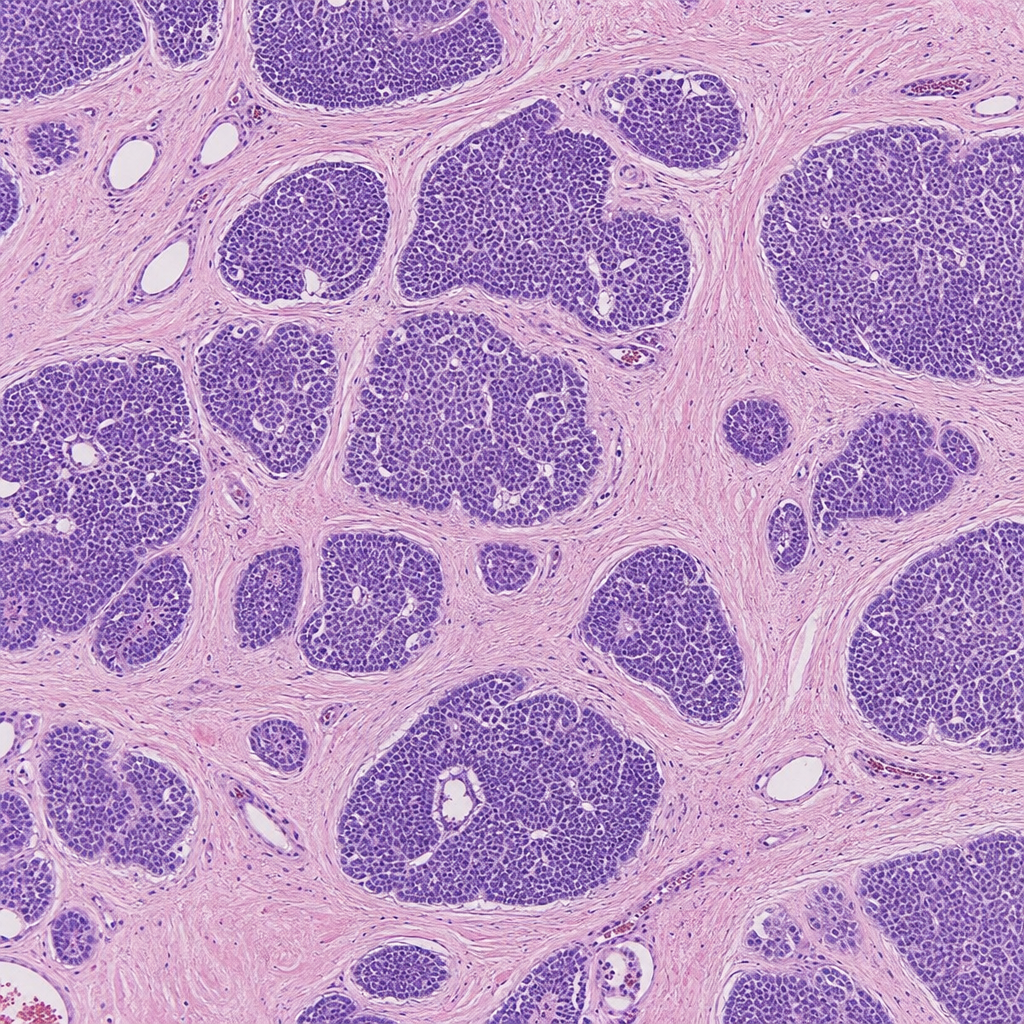
A skin biopsy from the scalp shows the histological pattern below. The pattern suggests the diagnosis as:
A 55-year-old woman complains that the skin of her armpits and groin is progressively darkening. Physical examination demonstrates velvety brown and waxy skin in the axilla and groin. Biopsy of these lesions shows a variably hyperplastic epidermis with many sharp peaks and valleys. Aside from cosmetic considerations, what is the primary medical significance of these lesions?
Which cytokeratin is characteristically expressed in Merkel cell carcinoma?
Which of the following is NOT a premalignant ulcer?
A 50-year-old fair-skinned male presented with an elevated plaque and an ulcerated, hyperpigmented nodule with variegation of color on his back, which has been progressively increasing in size. A biopsy of the skin lesion was performed. Which of the following antibodies can be tested for this condition?
What are the characteristic margins of squamous cell carcinoma?
Which of the following is a poor prognostic factor for melanoma?
Histological clefts in Lichen planus are described as:
What is the least common site for the spread of melanoma?
Practice by Chapter
Structure and Function of Skin
Practice Questions
Inflammatory Dermatoses
Practice Questions
Blistering Diseases
Practice Questions
Infectious Diseases of the Skin
Practice Questions
Disorders of Pigmentation
Practice Questions
Benign Skin Tumors
Practice Questions
Malignant Skin Tumors
Practice Questions
Connective Tissue Disorders of the Skin
Practice Questions
Cutaneous Manifestations of Systemic Disease
Practice Questions
Hair and Nail Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app