
Dermatopathology — MCQs

On this page
What is the most specific immunohistochemical marker for melanoma cells?
What is the characteristic histological feature of basal cell carcinoma?
Which stain is used for sebaceous cell carcinoma?
Which of the following is the site of malignant transformation of melanocytes in melanoma?
Which of the following is NOT true regarding the histopathology of psoriasis?
Hydropic degeneration of the basal cell of the stratum germinativum is a feature of which condition?
In the Clark's levels of tumor invasion for malignant melanoma, level 3 refers to which of the following?
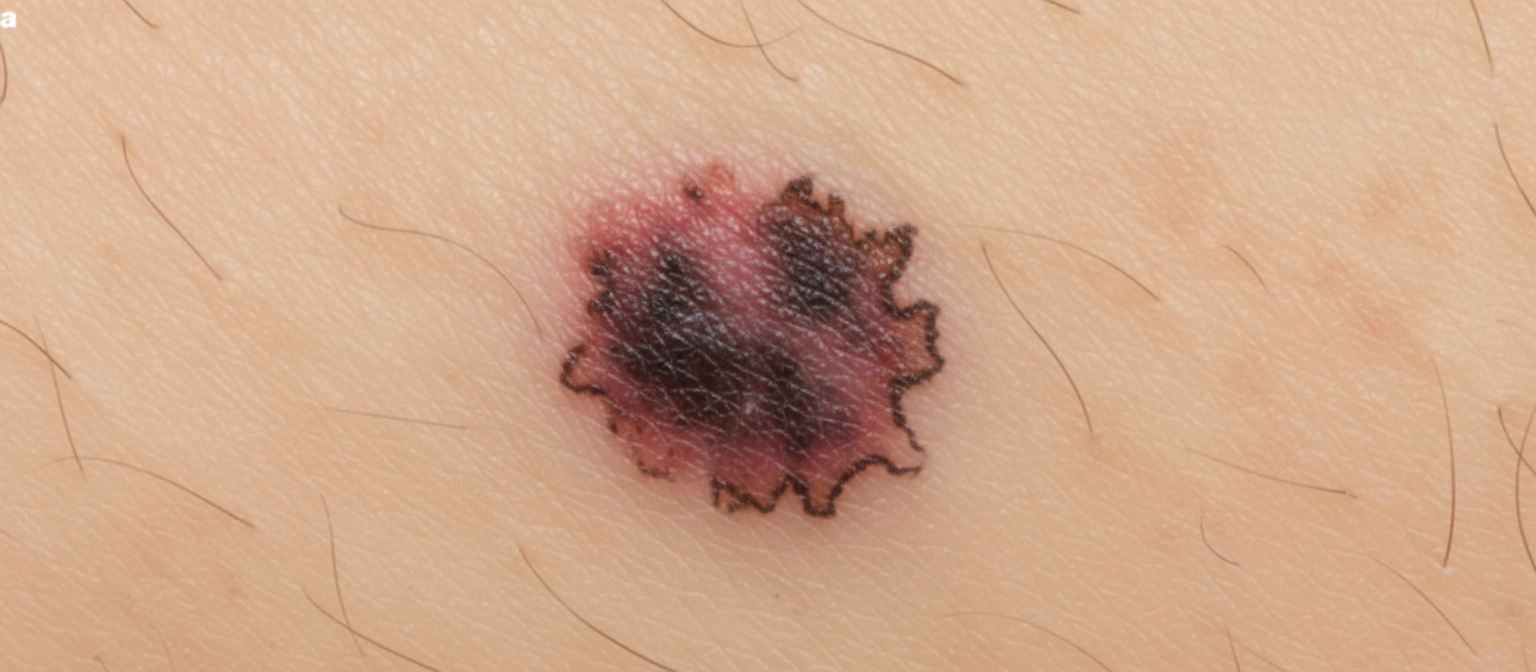
A 48-year-old woman presents with new-onset seizures and behavioral changes that began approximately 6 months ago. Advanced imaging reveals multiple round metastatic lesions in her brain. Her past medical history is remarkable for a black lesion on her toe that was excised 20 years prior. A thorough workup and multiple additional imaging studies reveal no primary malignancy. A lesion on the arm is noted and shown. Which of the following most likely characterizes this type of malignancy?
Melanoma staging according to which classification?
Which of the following is a marker for Melanoma?
Practice by Chapter
Structure and Function of Skin
Practice Questions
Inflammatory Dermatoses
Practice Questions
Blistering Diseases
Practice Questions
Infectious Diseases of the Skin
Practice Questions
Disorders of Pigmentation
Practice Questions
Benign Skin Tumors
Practice Questions
Malignant Skin Tumors
Practice Questions
Connective Tissue Disorders of the Skin
Practice Questions
Cutaneous Manifestations of Systemic Disease
Practice Questions
Hair and Nail Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app