
Trauma — MCQs

On this page
Which is the suggested treatment of the lesion shown in the X-ray?

An elderly patient slipped in the bathroom and sustained injury over the hip joint. X- Ray is shown below. Her attitude of leg will be?

What type of fracture is shown in X-ray of left shoulder?

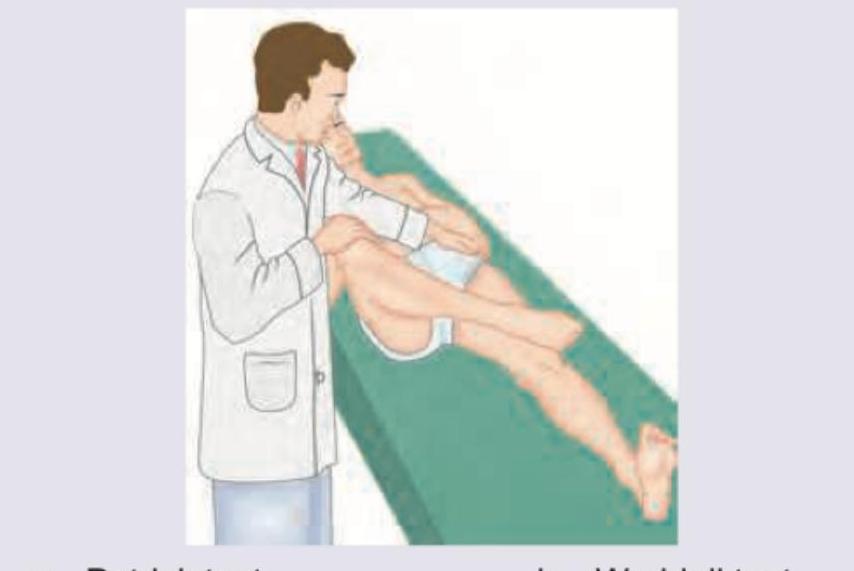
What is the test being performed in the patient?
Consider the following : 1. Pain relief 2. Prevention of infection 3. Anaesthesia 4. Restoration of anatomy Which of the features given above are priorities for fracture treatment?
The commonest complication of fracture of clavicle is :
The nerve most likely to get injured in patients with fracture of upper end of radius is :
Which one of the following fractures is most often complicated by fat embolism ?
Avascular necrosis may develop in the following fractures except
What is the most common injury sustained due to fall on outstretched hand by a person aged 65 years?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app