
Trauma — MCQs

On this page
Spot the diagnosis:

What is the grade of fracture according to Garden's classification?

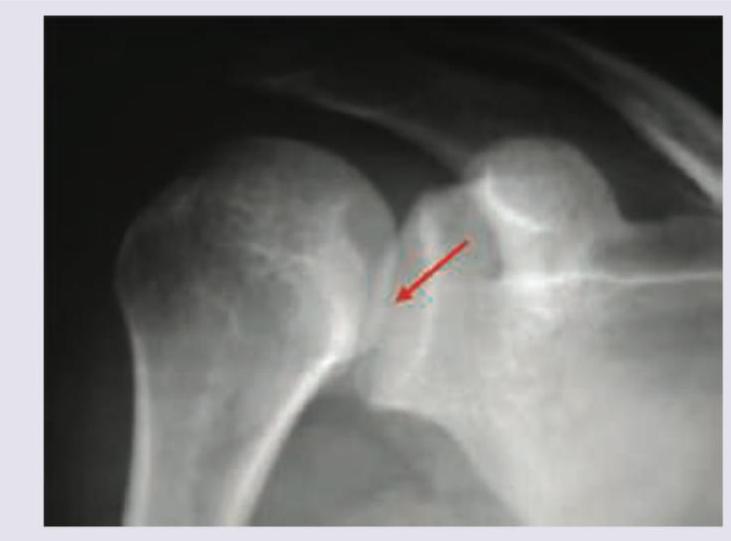
All are correct about the condition shown in X-ray except:

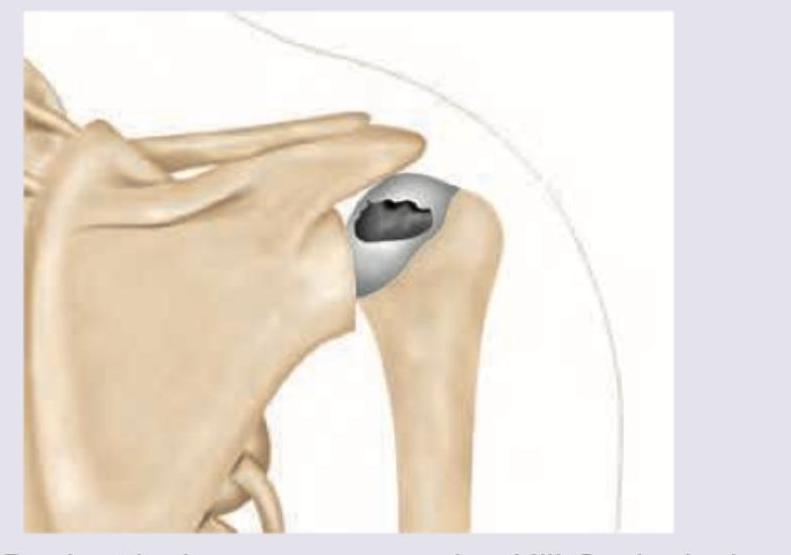
An epilepsy patient presents in postictal period with inability to touch opposite shoulder. What is incorrect about the diagnosis?
A 65-year-old woman falls on an extended and outstretched hand while walking her grandchild to school. She presents to the emergency department in severe pain and is holding her left wrist. On examination, there is swelling, tenderness, and deformity of the wrist. Which of the following is the most likely diagnosis?

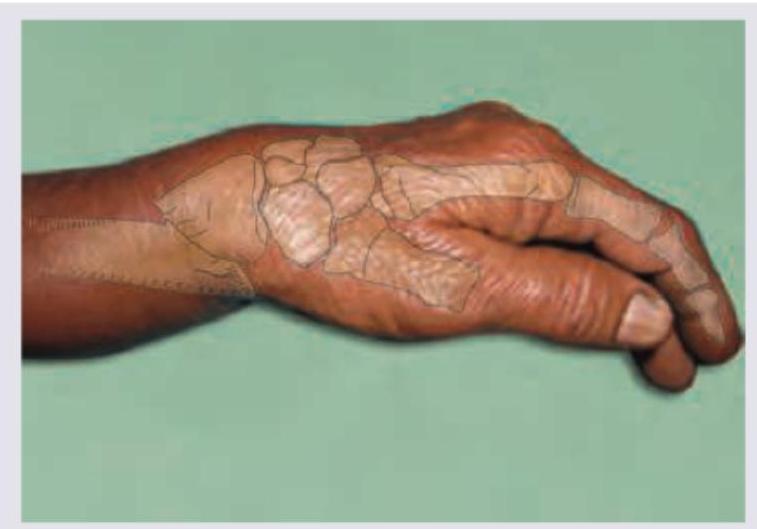
Which is incorrect about the image shown below?
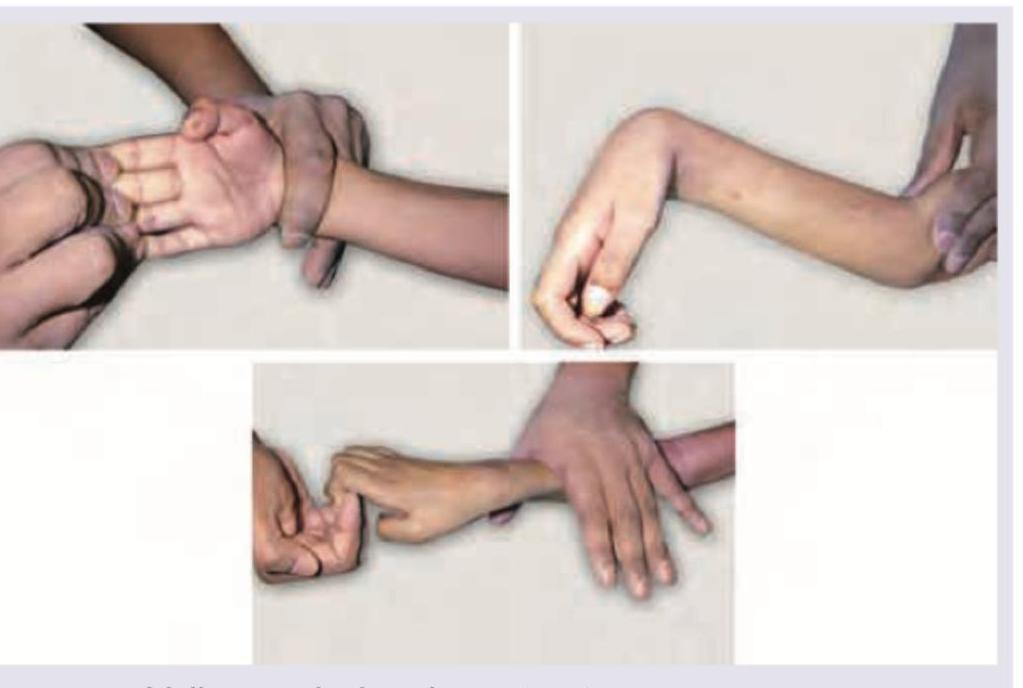
Comment on the diagnosis based on examination findings shown below: (Recent NEET Pattern 2016-17)
A 55-year-old woman tripped over a piece of banana and sustained a fracture shown below. Diagnosis is:

A 50-year-old orthopaedics doctor went for sky diving while vacationing abroad. On return he had the following physical finding. What is the diagnosis?

Comment on the diagnosis:
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app