
Trauma — MCQs

On this page
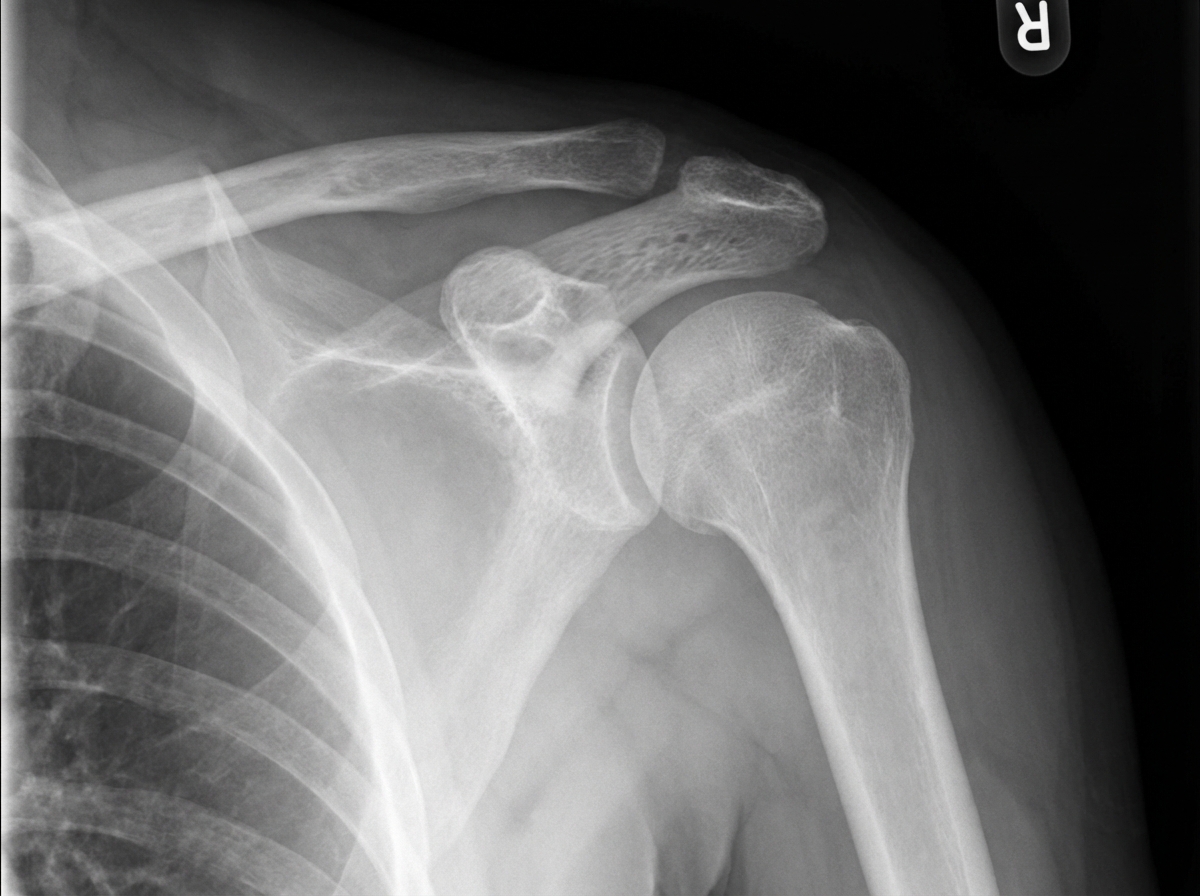
Which of the following statements regarding this diagnosis is true?
A 37-year-old female patient has a fracture of the clavicle. The junction of the inner and middle third of the bone exhibits overriding of the medial and lateral fragments. The arm is rotated medially, but it is not rotated laterally. Which of the following complications is most likely to occur secondary to the fractured clavicle?
Which of the following is NOT a recognized feature of myositis ossificans?
Which of the following statements regarding supracondylar fracture of the humerus in children is true?
What is a fracture of the 5th metatarsal called?
A student presents with a shoulder injury sustained while playing football. On comparing the symmetry of his two shoulders, a marked elevation of the distal end of the clavicle with respect to the acromion is noted on the injured side. X-ray examination reveals a grade III shoulder separation. Which ligament must be torn for this injury to have occurred?
What is the most common dangerous complication of posterior dislocation of the knee?
Fracture of the neck of the fifth metacarpal bone occurs in which type of fracture?
What is Jones fracture?
A 21-year-old male with a fracture of the surgical neck of the humerus presents with a regimental badge sign and difficulty in abduction. What is the most likely nerve injury?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app