
Trauma — MCQs

On this page
A 32-year-old male with a history of seizures presents with pain in the left shoulder region. The left upper limb is addicted and internally rotated. What is the diagnosis?
Recurrent dislocation of the shoulder is most commonly associated with which type?
All of the following statements regarding mandibular fractures are true EXCEPT:
What is the most common type of hip dislocation?
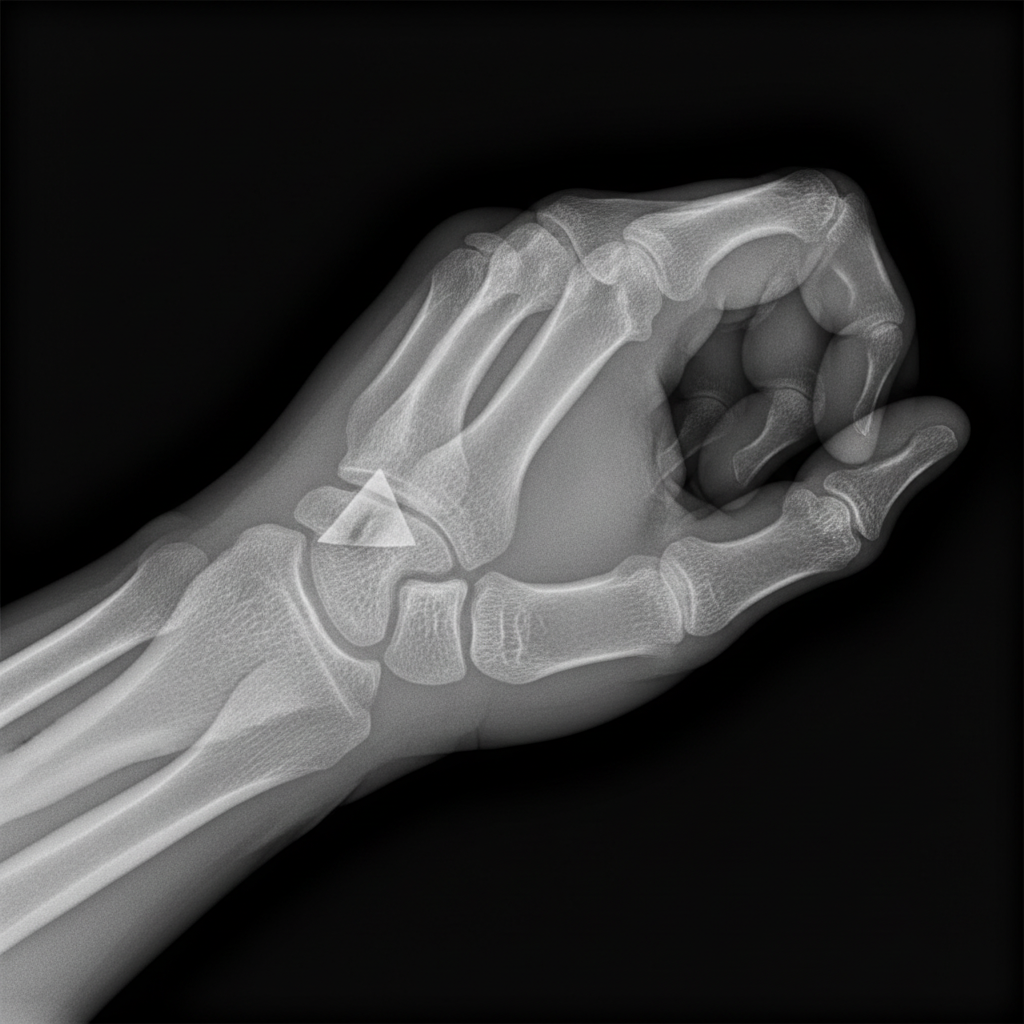
Fracture shown in this radiograph is:
Which of the following is referred to as Luxatio erecta?
Tardy ulnar nerve palsy is commonly seen in?
The vascular sign of Narath is positive in which of the following?
What is the best treatment for a trochanteric fracture of the femur?
Which complication may arise after a supracondylar fracture?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app