
Trauma — MCQs

On this page
A 60-year-old man who fell in the bathroom and is unable to stand on his right buttock region due to ecchymosis, with external rotation of the leg and the lateral border of the foot touching the bed. The most probable diagnosis is:
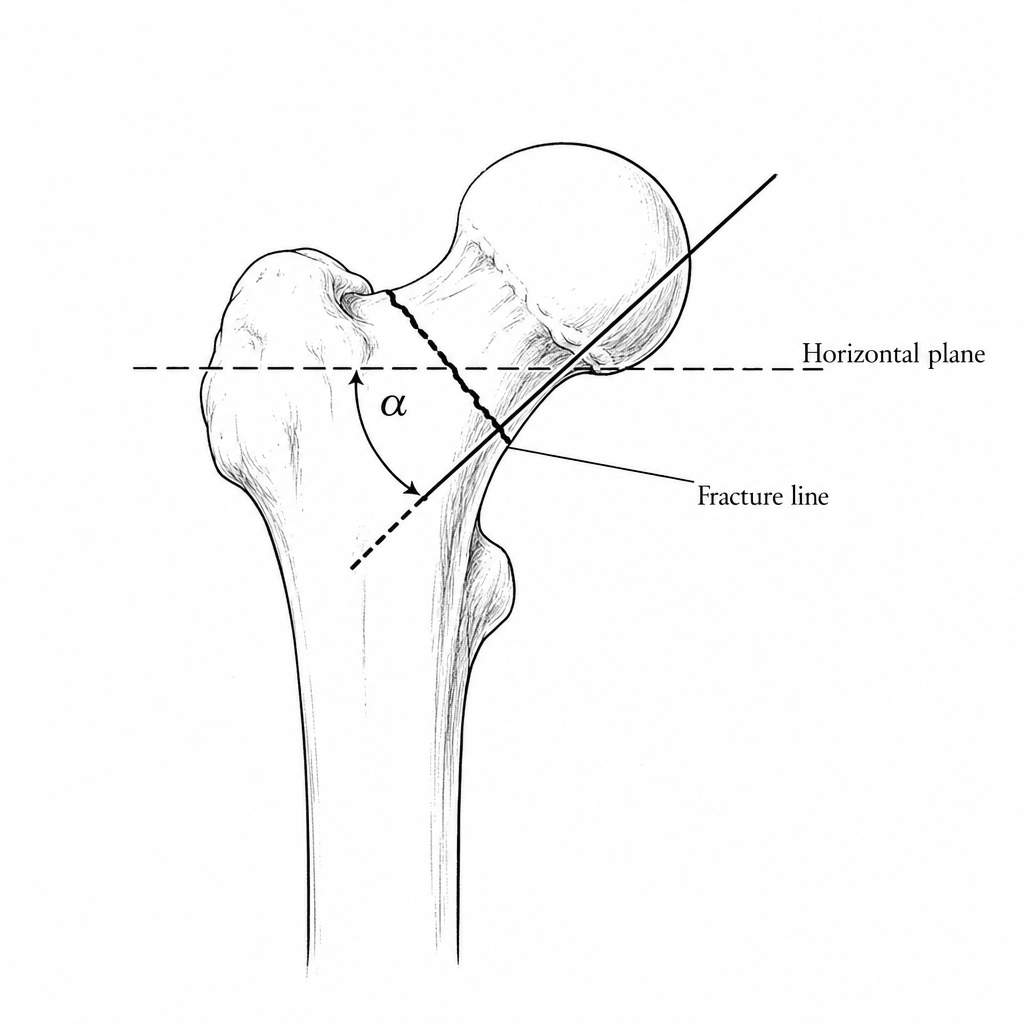
What is the angle formed by joining a line extended from the fracture line of the fracture neck to an arbitrary line depicting the horizontal plane?
A patient presents with a compound fracture of the tibia, with a 1-cm opening in the skin. Which grade does it belong to?
Subtrochanteric fractures of the femur can be treated by all of the following methods, except:
Which of the following is NOT a primary goal of open reduction and internal fixation (ORIF)?
Which of the following is a contraindication for open reduction & internal fixation (ORIF)?
Avascular necrosis (AVN) is commonly associated with which type of femoral neck fracture?
Which of the following is not considered an emergency treatment for acetabular fractures?
What is the acceptable angle of reduction for a tibial fracture?
In which type of fracture is closed pinning not typically performed?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app