
Trauma — MCQs

On this page
A 28-year-old male presents with a crush injury to the leg. His leg is swollen, and he experiences severe pain with passive stretching of the toes. What is the next best step in management?
What is the most common complication of a posterior shoulder dislocation?
What factors should be considered when deciding between limb salvage surgery and amputation for a patient with a severe traumatic injury to the lower extremity?
A 10-year-old child presents with a distal radius fracture showing a 'dinner fork' deformity. What is the most characteristic feature of this type of fracture?
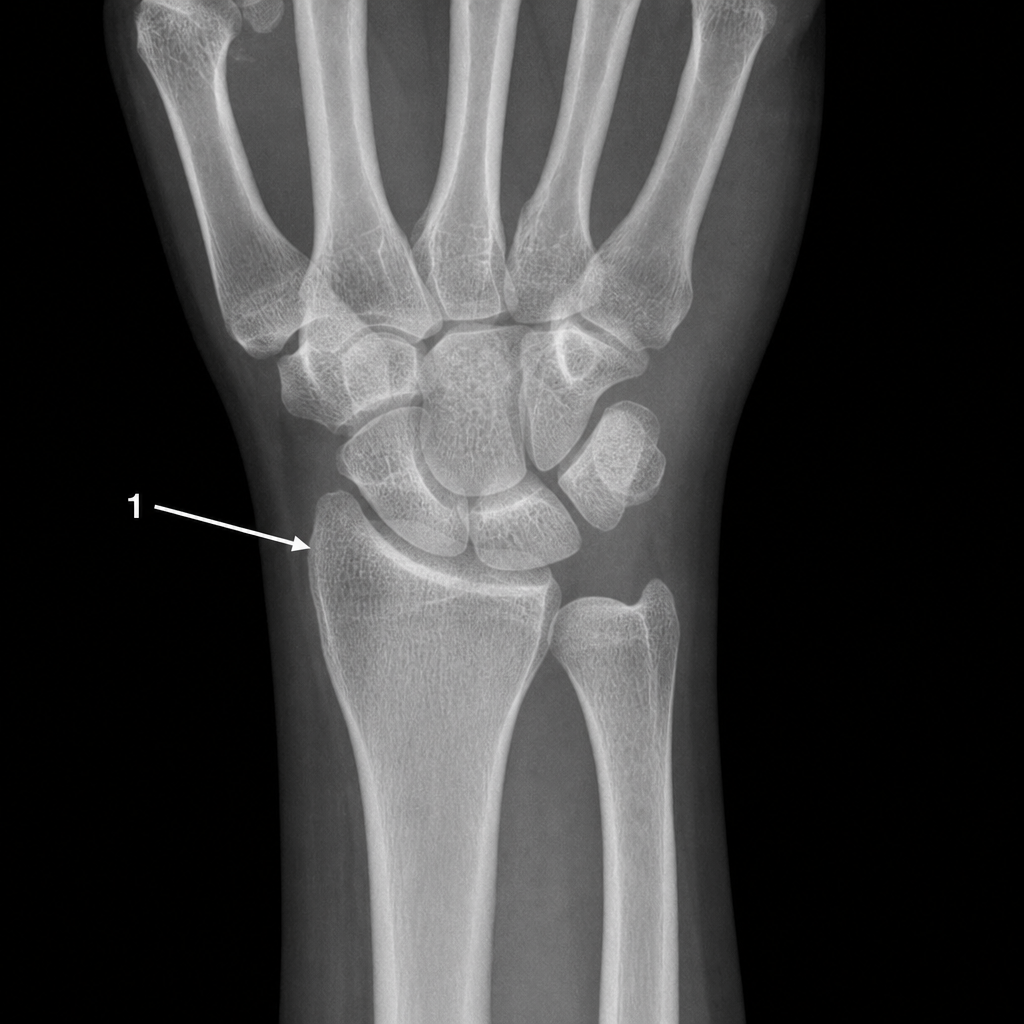
Identify the bone numbered in the X-ray that most commonly fractures when a person falls on outstretched hands.
Palpable femur head on per rectal exam is a feature of which of the following conditions?
What is the absolute pressure threshold for surgical intervention in compartment syndrome?
Management of displaced non comminuted intercondylar humerus fracture is?
Which of the following statements about Galeazzi fracture dislocation is incorrect?
Dunlop traction is a type of traction used in the management of?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app