
Trauma — MCQs

On this page
Which of the following requires emergency treatment?
Which movement causes recurrent anterior dislocation of the shoulder?
Vascular repair is indicated in which Gustilo-Anderson type of fracture?
Which of the following fractures is not managed by compression screws?
What is the typical position of the leg in a fracture of the neck of the femur?
Management of calcaneal fractures depends upon which of the following?
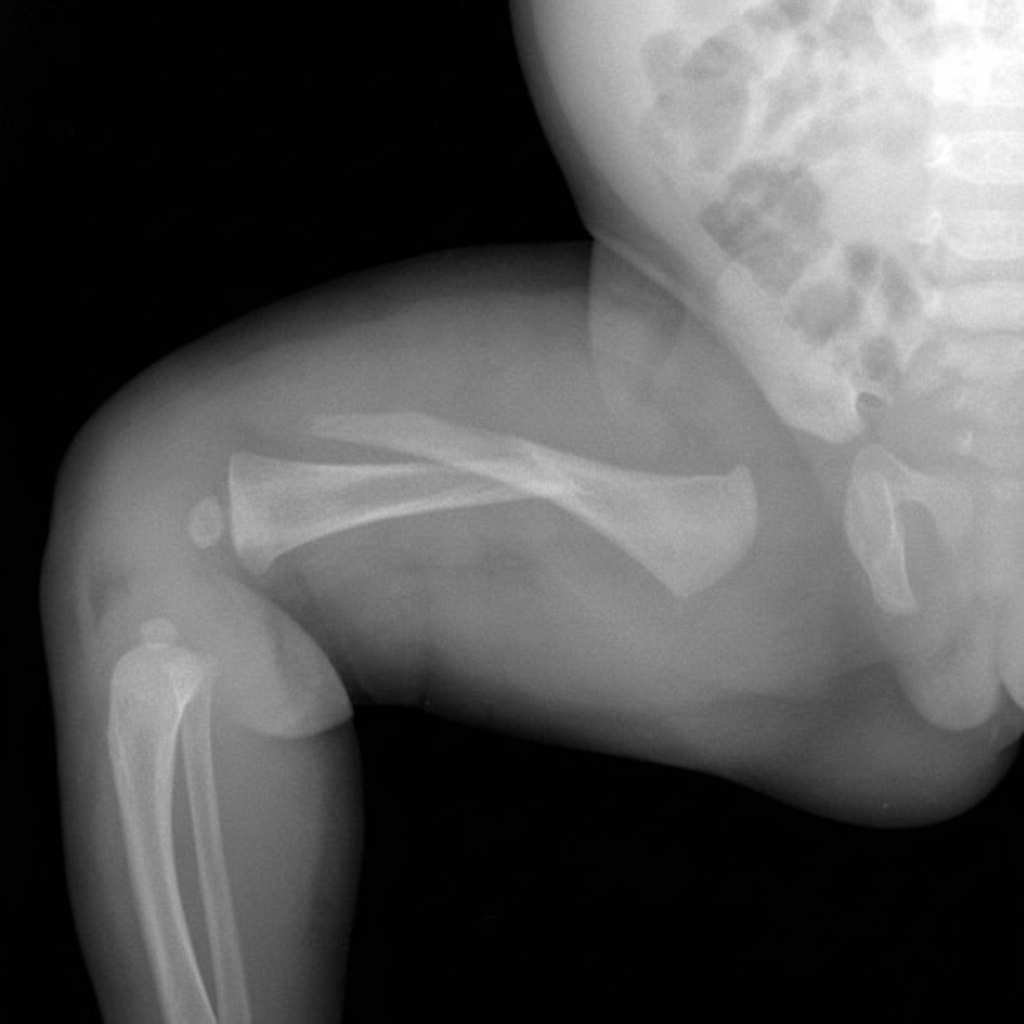
Which nerve is most at risk in the injury shown in the accompanying radiograph?
Which of the following elbow injuries involves the three-point relationship?
What are the complications of fracture of the radius?
Which of the following positions is classically seen in posterior dislocation of the hip?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app