
Trauma — MCQs

On this page
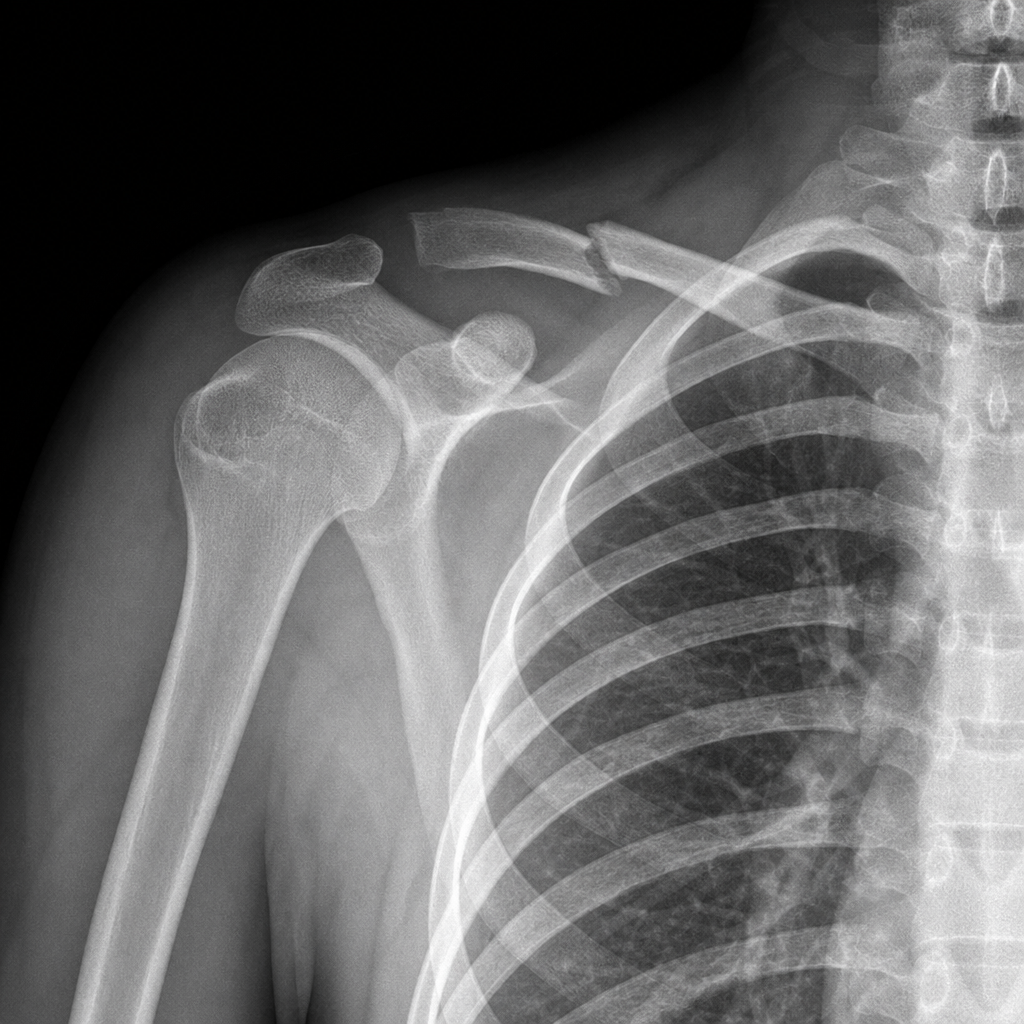
A patient received an electric shock and fell down. He cannot do external rotation of shoulder and cannot move arm. What is the diagnosis:-
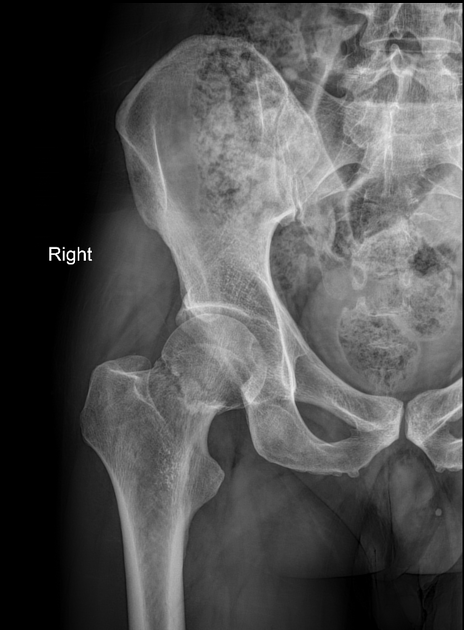
79 yrs old lady had fall, the following X-ray was taken. Which of the following is treatment?
A boy was riding bicycle, he fell down forward and injury to his shoulder was seen, which nerve injury will be seen in the condition as given in X-ray?
In fracture of upper 1/3 of forearm, it is immobilized in:
A 40-year-old patient presents with a femur fracture, pulmonary infiltration, and respiratory distress. What is the most likely diagnosis?
Post-menopausal woman, fell down in washroom. What is the most common fracture she may suffer?
Lauge - Hansen classification belongs to:-
Posterior interosseous nerve is injured in
Which type of fracture is most likely to cause exsanguinating blood loss?
All of the following are indications for open reduction and internal fixation (ORIF) of fractures EXCEPT:
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app