
Trauma — MCQs

On this page
Indications for fasciotomy in compartment syndrome include all EXCEPT:
Identify the implant shown in the image:

A patient fell off a bicycle and now complains of pain around the hip, with shortening of the affected limb. The hip is held in a position of flexion, adduction, and internal rotation. What is the most likely diagnosis?
What should be done as an immediate measure for ongoing bleeding in a patient with pelvic bone fracture?
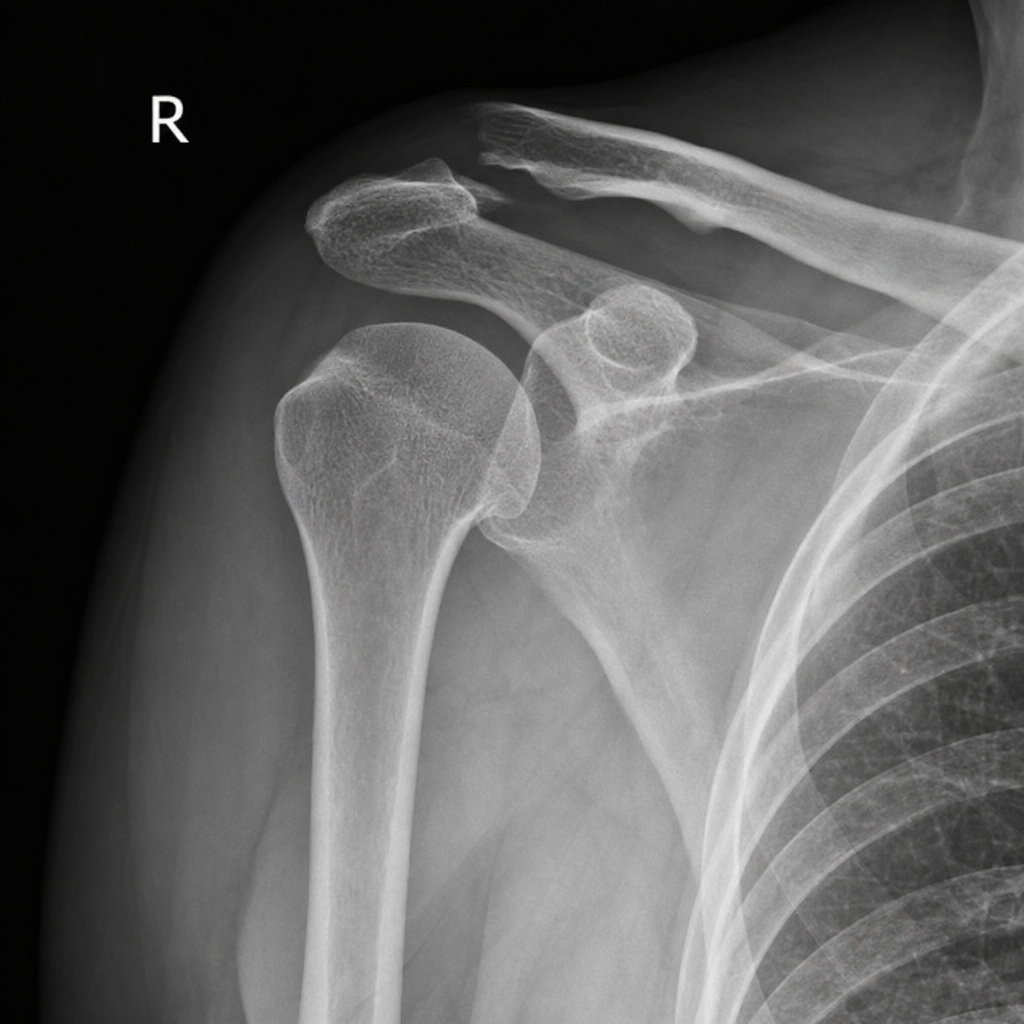
A 40 year male patient presented to the ER with a history of fall and C/O pain and swelling in right shoulder region. The x-ray of the patients suggests tear in which of the following ligaments? (Select all that apply)
Following a femoral shaft fracture, your consultant asks you to provide tibia traction. Which of the following will you request from the nurse? 1. Thomas splint 2. K-wire 3. Steinmann pin 4. Denham's pin 5. Bohler's stirrup 6. Bohler Braun splint
Which of the following findings appear late in compartment syndrome?
A 30-year-old male presents with pain and limited movement in his shoulder following a fall. X-ray reveals an anterior dislocation of the glenohumeral joint. Which of the following structures is most likely to be damaged in this injury?
Most common complication of extra capsular fracture of neck of femur is:
Which nerve is commonly damaged in fracture of neck of fibula?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app