
Trauma — MCQs

On this page
What is the preferred treatment for an inter-trochanteric fracture in a 72-year-old female?
A 25-year-old man presents to the emergency department following a motorbike accident and is found to have a closed midshaft fracture of the left tibia. Six hours later, he develops severe leg pain that is disproportionate to the injury and worsens with passive dorsiflexion of the foot. The pain is not relieved by analgesics. On examination, dorsalis pedis and posterior tibial pulses are present, but there is no sensation over the first dorsal webspace. What is the most appropriate next step in management?
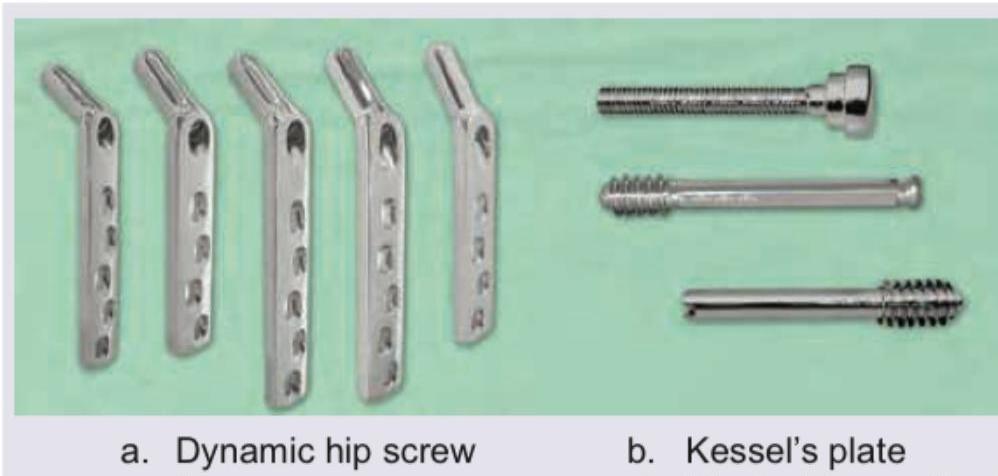
What does the implant labeled 'b' in the given image show?
Identify the fracture shown in the image below:

Which of the following classifications is used to assess the fracture shown below?

Serial X-rays taken over 6 months after sustaining a fracture show no progression of healing. What is the diagnosis?

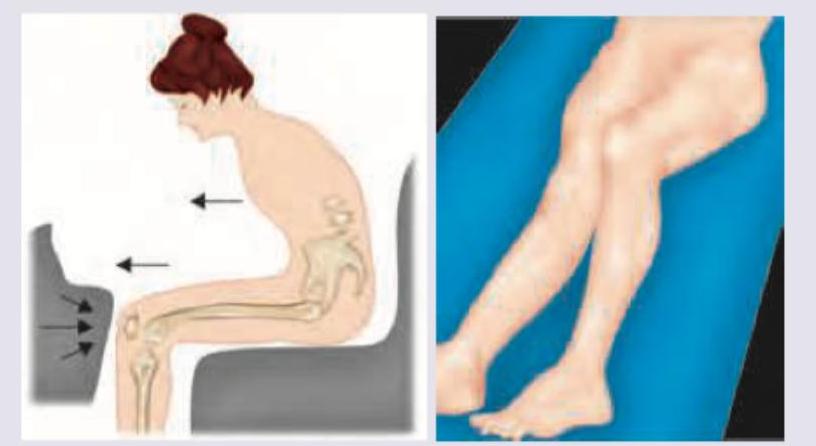
Which of the following is most commonly seen after the accident shown?
What is the name of the splint shown here?

Spot the diagnosis:

What is the grade of fracture according to Garden's classification?

Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app