
Trauma — MCQs

On this page
A 37-year-old male is brought to the emergency room after a road traffic accident. On examination, the capillary refilling time is delayed in the left lower limb. Which of the following is NOT an indication for amputation in this patient?
A child presents with a fracture of the distal end of the radius after playing cricket. The fracture was treated with a plaster of Paris cast. Which of the following is a recognized late complication of a Colles fracture?
Pipkin classification is used for which type of fracture?
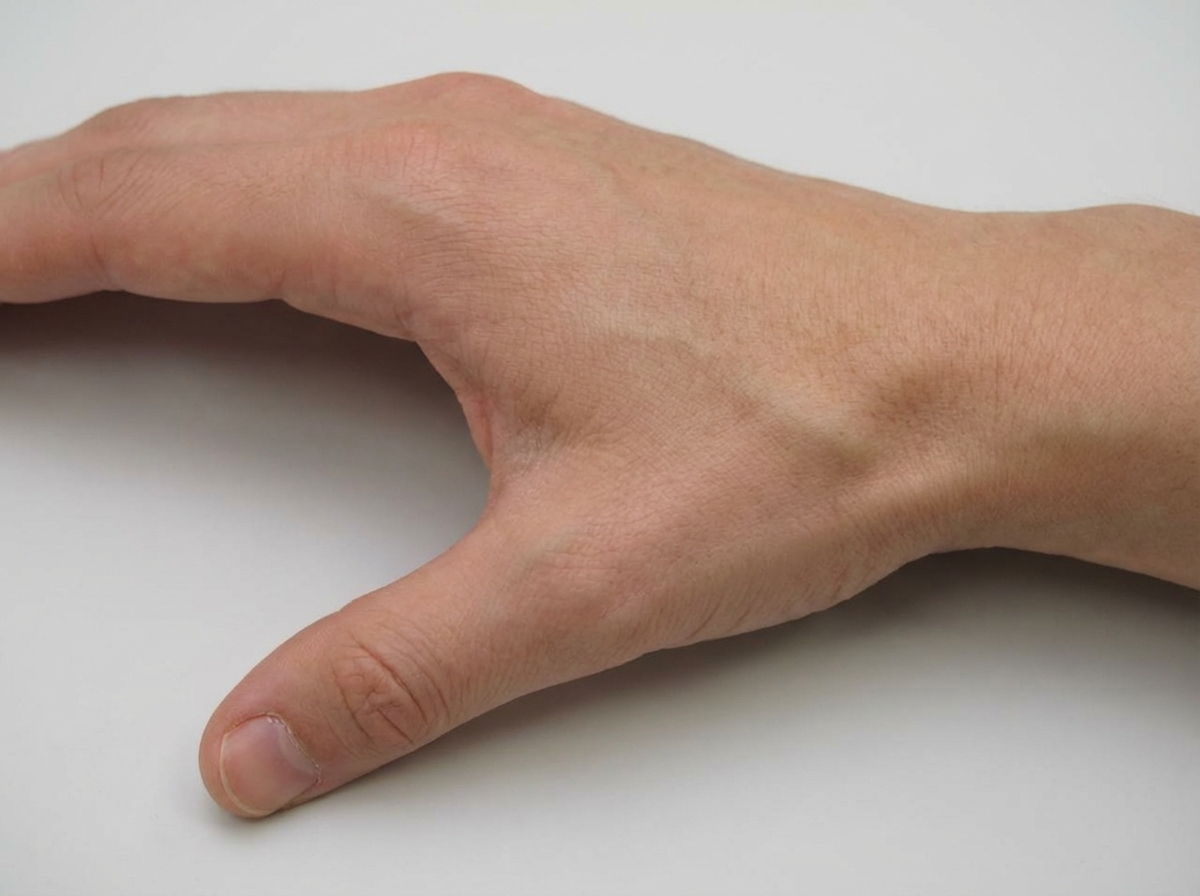
A patient falls on an outstretched hand and presents with tenderness in the shown area. Which bone is most commonly fractured?
Non-union is a complication of which of the following fractures?
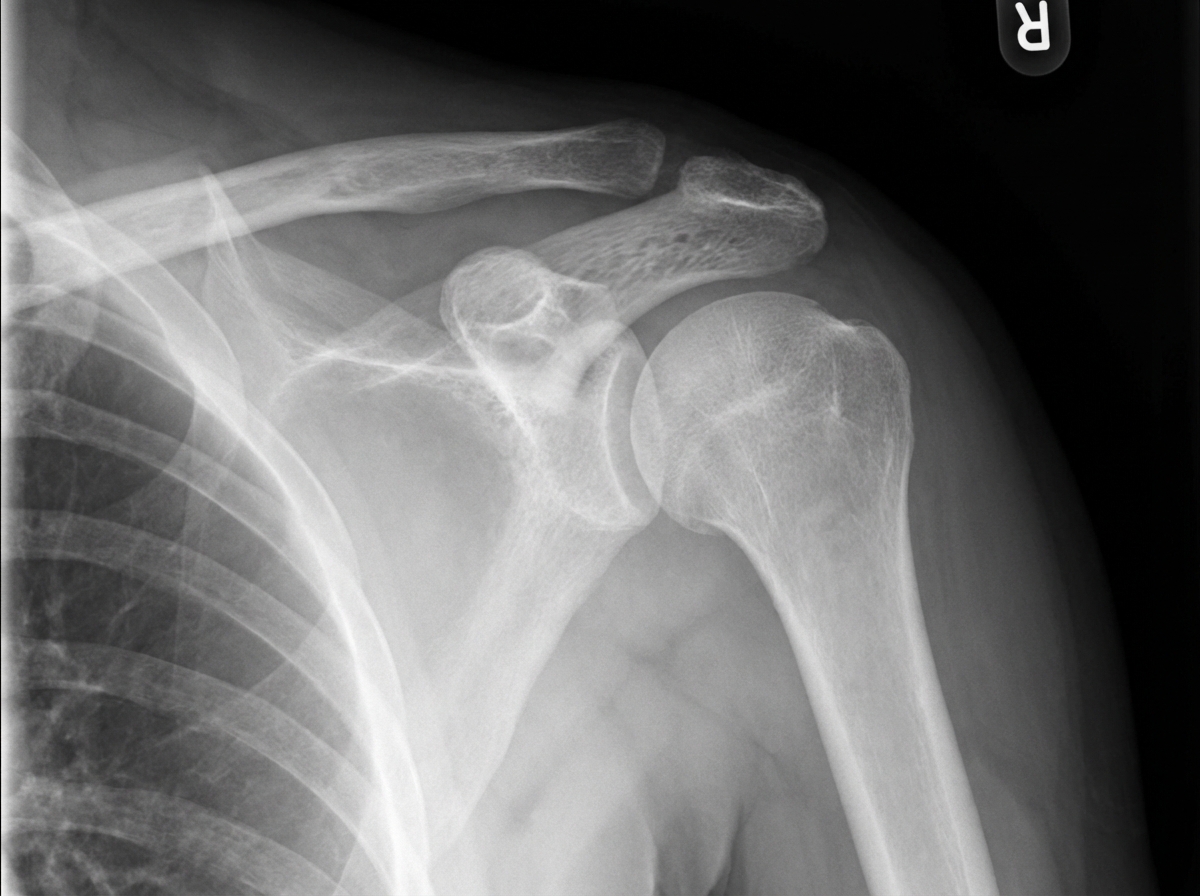
All of the following statements about dislocation of the shoulder are true, except?
A 45-year-old female has a history of a slip in the bathroom, complaining of right hip pain and tenderness in Scarpa's triangle. The X-ray is normal. What is the next investigation?
Which is the most commonly injured tarsal bone?
The posterolateral lesion in the head of humerus in cases of recurrent anterior shoulder dislocation is:
Which of the following statements regarding this diagnosis is true?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app