
Trauma — MCQs

On this page
Which of the following are considered non-rigid fixation devices?
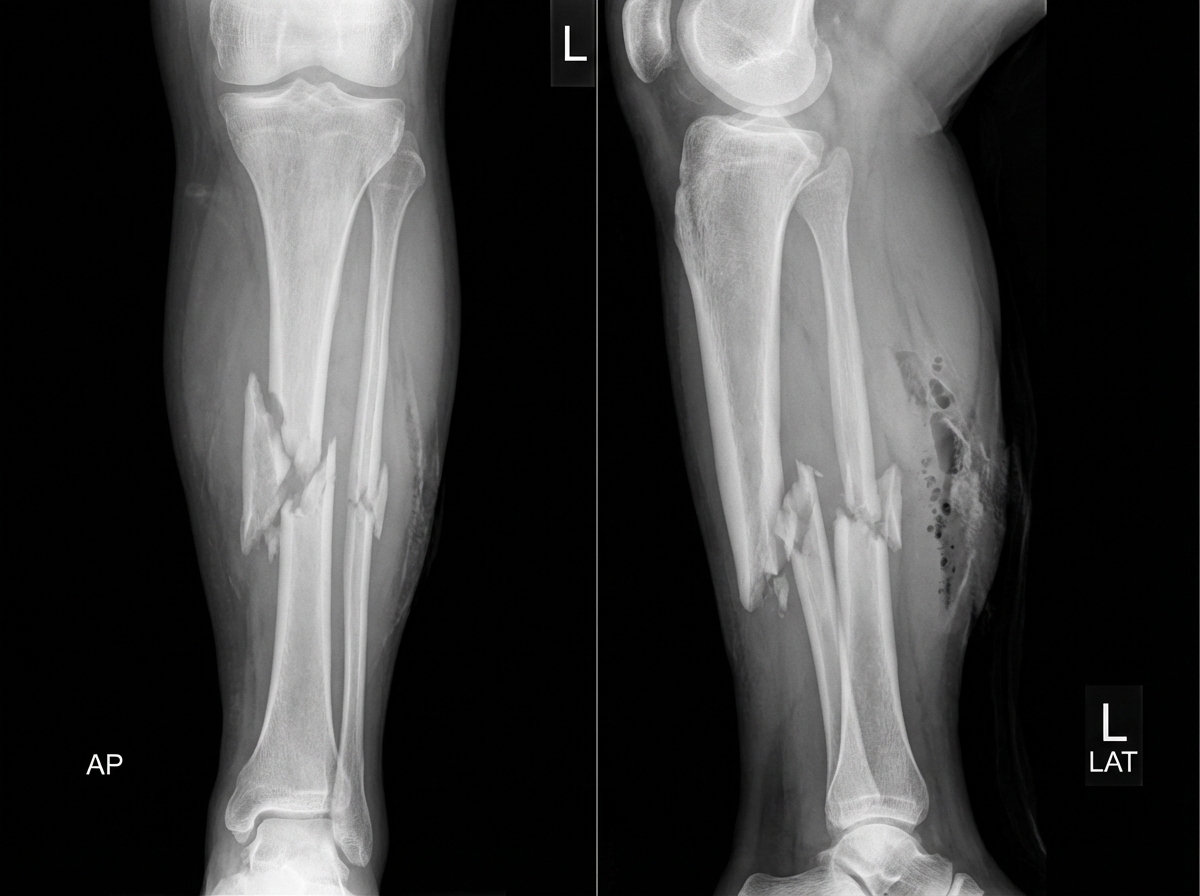
A 22-year-old man is brought to the emergency department following a rugby injury. Which of the following statements is false regarding the fracture shown?
What is the maximum weight typically allowed in skeletal traction?
A 23-year-old male basketball player presents with a shoulder injury sustained during a game. Physical and radiographic examinations were performed. Which of the following structures has most likely been torn?

A 23-year-old man involved in an accident is brought to the emergency room with a displaced fracture of the distal third of his left humeral shaft. On his right side, he has a displaced fracture of the surgical neck of his humerus as well as a fracture of the medial epicondyle of his distal humerus. He complains of pain in both arms and the inability to move parts of his hand. On physical examination, his arm is swollen with a deformity at the corresponding parts of his humerus. His motor examination is abnormal. Which of the following muscles will this patient most likely have trouble using secondary to the nerve injury sustained in his accident?
A 17-year-old high school tennis player sustains a right midshaft clavicle fracture. Which of the following increases the risk of nonunion in non-operative treatment of clavicle fractures?
What is a floating knee?
A 34-year-old woman sustained a direct blow to the patella from the dashboard during an automobile crash. Radiographic examination reveals patellofemoral syndrome, characterized by lateral dislocation of the patella. Which of the following muscles requires strengthening through physical rehabilitation to prevent future dislocations?
In Volkmann's ischemic contracture, what is the recommended timeframe for surgical intervention?
Which of the following arteries is affected in anterior shoulder dislocation?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app