
Trauma — MCQs

On this page
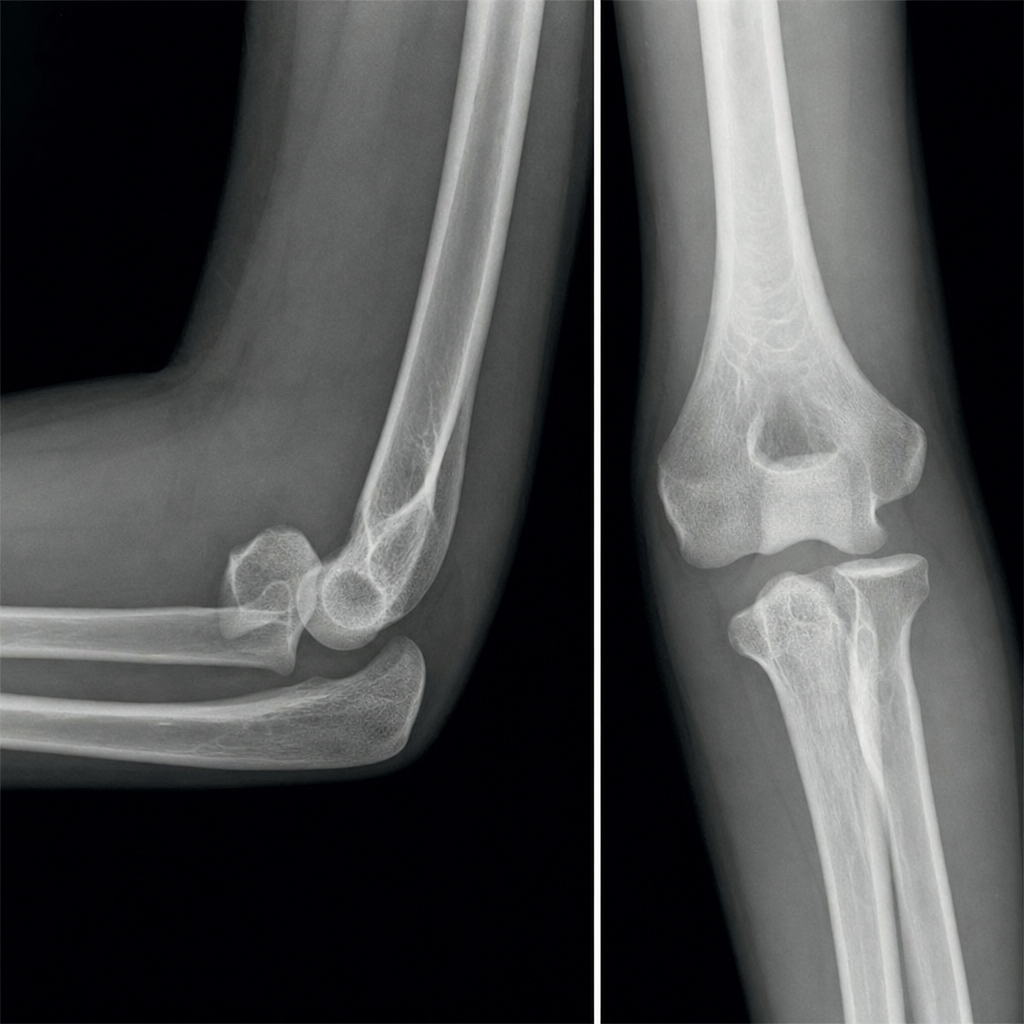
A 24-year-old woman fell while ice-skating. What abnormality is shown?
Maximum shortening of limbs occurs in which condition?
In a 70-year-old lady with an intracapsular fracture of the neck of femur, what is the ideal treatment?
Which is the most frequently dislocated joint in the body?
Which of the following statements is not true regarding traction?
Meyer's procedure is a method for treatment of which of the following conditions?
A 5-year-old boy presents with a fracture in the shaft of the humerus. How will you exclude the involvement of the radial nerve?
A 30-year-old male patient presents with breathlessness, irritability, and confusion. He has a history of a fracture of his right arm 3 days ago. On physical examination, a diffuse petechial rash is seen. Blood examination reveals thrombocytopenia. What is the most likely diagnosis for this patient?
What is true about post-traumatic fat embolism syndrome?
What is the treatment for a severely comminuted fracture of the patella that cannot be reduced?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app