
Trauma — MCQs

On this page
What is the management for the depicted condition?

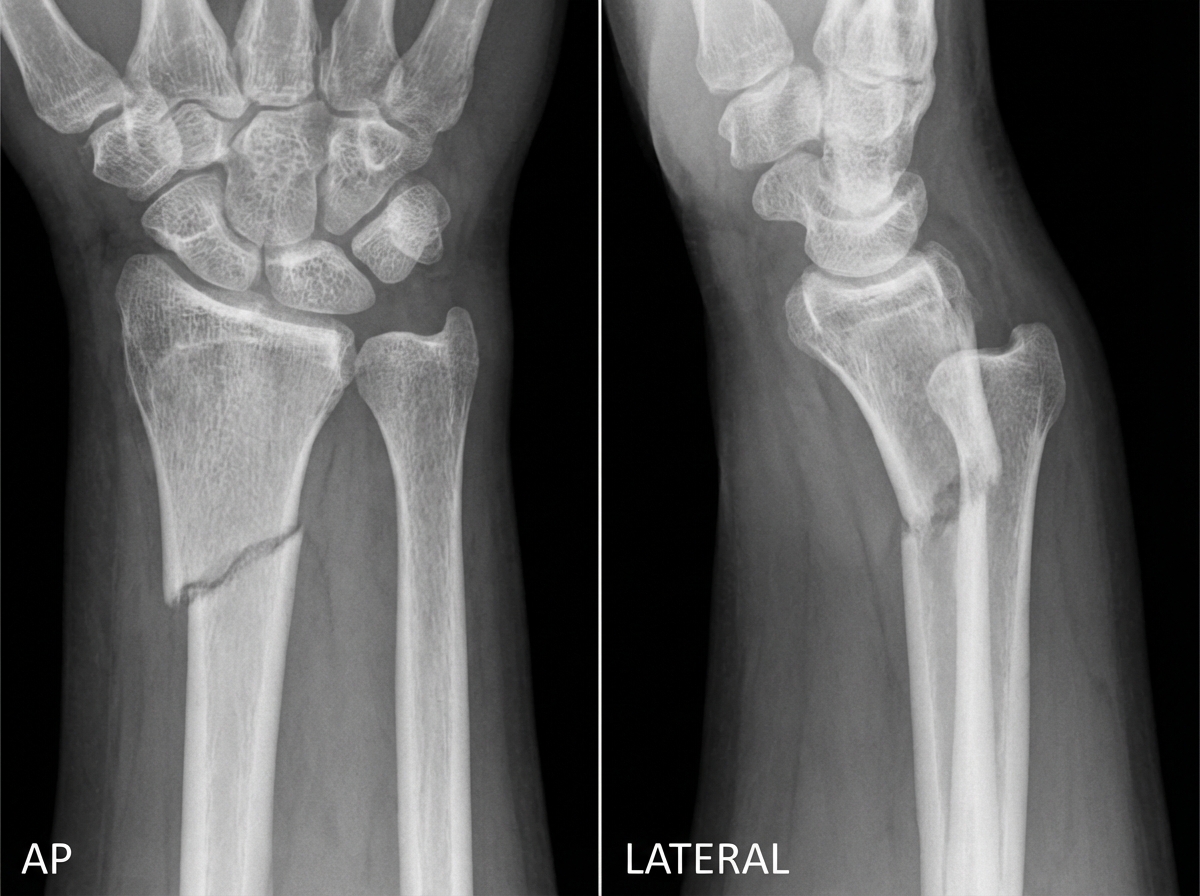
A patient presents with a fall on an outstretched hand. An X-ray is shown below. Which of the following vessels is most likely involved?

AP and lateral views of the wrist are provided. What is the diagnosis?
Volkmann's Ischaemic Contracture is due to which of the following?
Stress fracture is treated by:
A 20-year-old male presents with anterior shoulder dislocation. This injury is usually caused as a combination of which of the following?
Functional cast bracing is NOT used in which of the following fractures?
Which of the following is true about Colles' fracture?
In Volkmann's contracture, which artery is injured?
Which of the following statements regarding fracture of the clavicle is true?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app