
Trauma — MCQs

On this page
Which of the following is a complication of a talar fracture?
A 60-year-old female presents after a fall in the bathroom, unable to stand. On examination, her right leg is in external rotation, with limited movement and tenderness in Scarpa's triangle. There is no history of fever. X-ray shows no fracture line. What is the next step in management?
What is the earliest sign of compartment syndrome of the leg?
Which among the following patients with a fracture requires the 1st priority to be informed to a senior?
Fat embolism syndrome is characterized by which of the following?
Nonunion is a very common complication of intracapsular fractures of the neck of femur. Which of the following is not a very important cause for the same?
All of the following are indications for open reduction and internal fixation of fractures except?
What is the permissible ischemia time for proximal limb amputations?
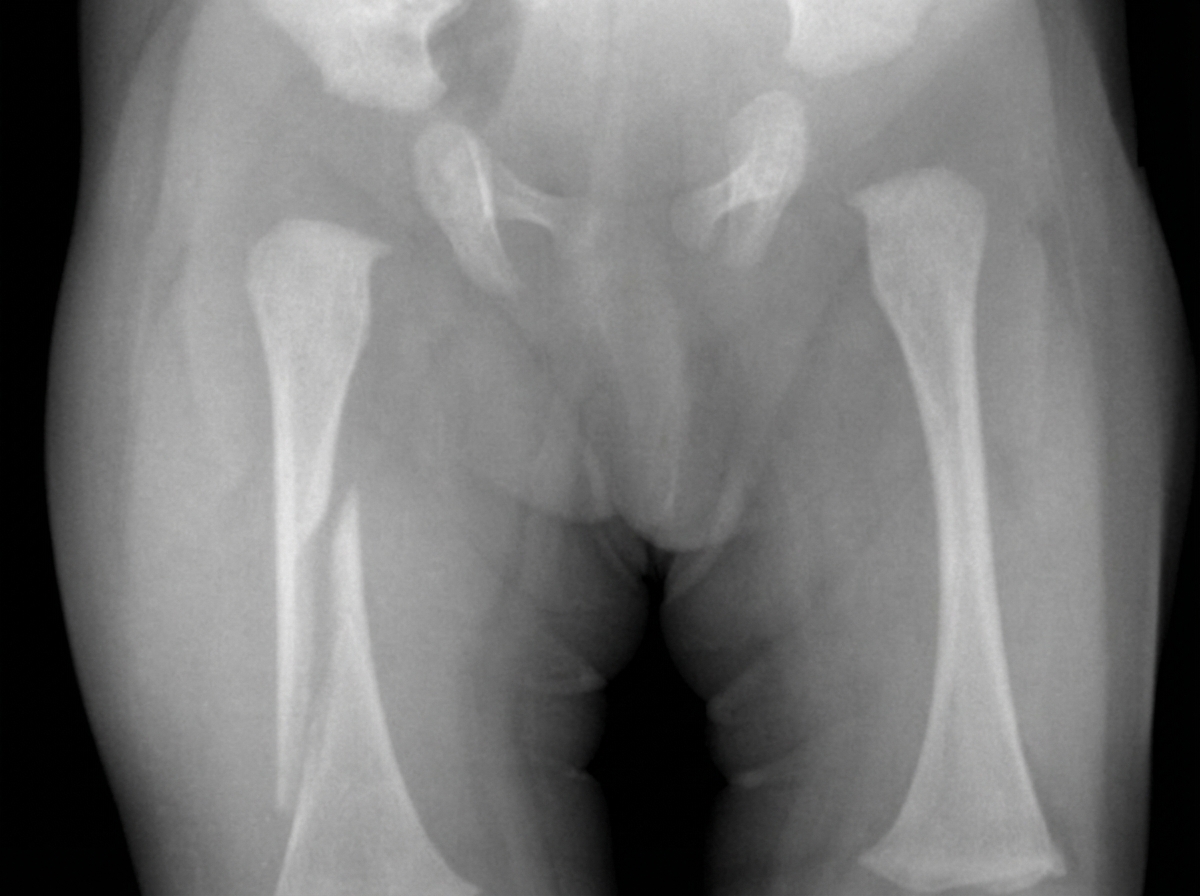
On the AP radiograph, where is the right femoral fracture centered?
All of the following show compression osteosynthesis except:
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app