
Trauma — MCQs

On this page
What is a Colles fracture?
What is the initial management for an open fracture?
All of the following factors evaluate the chances of amputation in a limb, except?
Early recovery of Sudeck's atrophy can be best managed by which of the following interventions?
Arrange the following nerves according to the incidence of their involvement in a supracondylar fracture of the humerus:
A 35-year-old male presents after a direct blow to the knee. Radiograph shows a displaced transverse patellar fracture with a gap of 4 mm and disruption of the extensor mechanism. What is the treatment modality of choice?
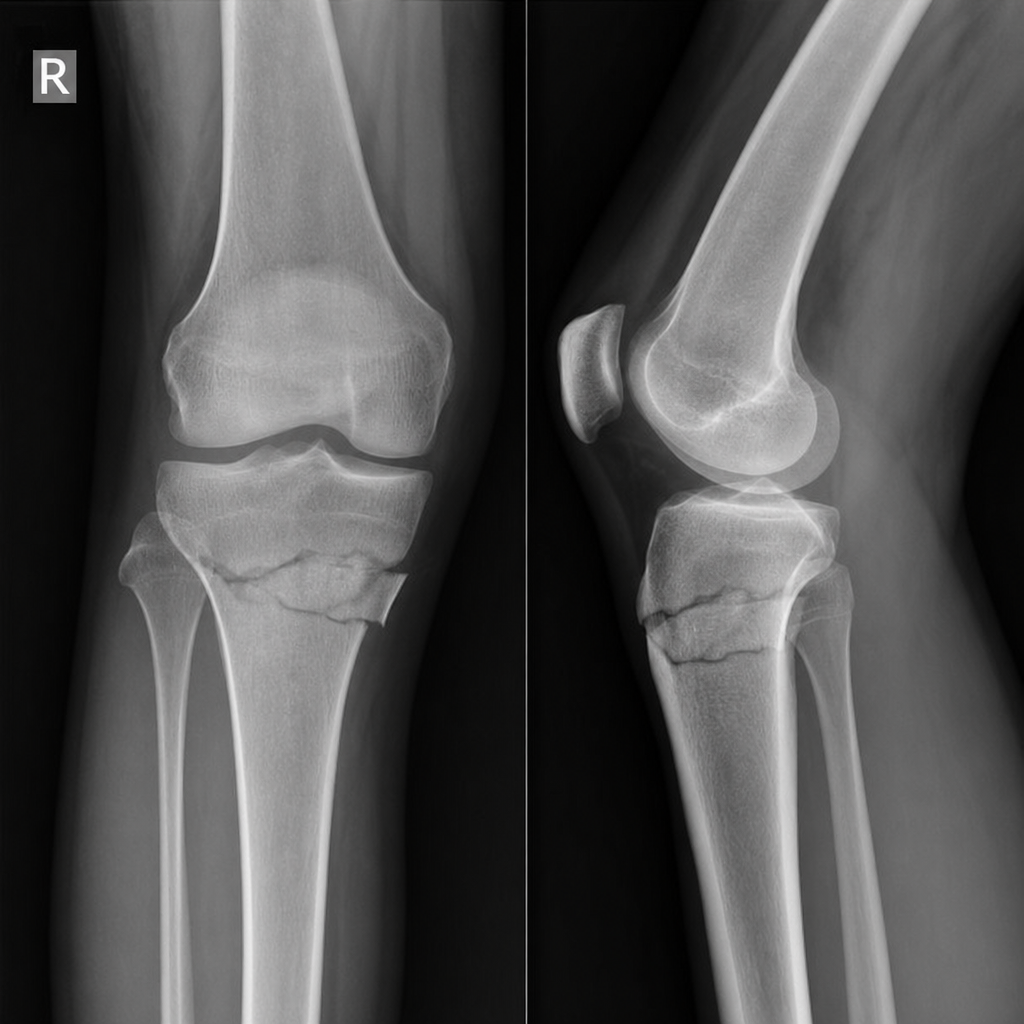
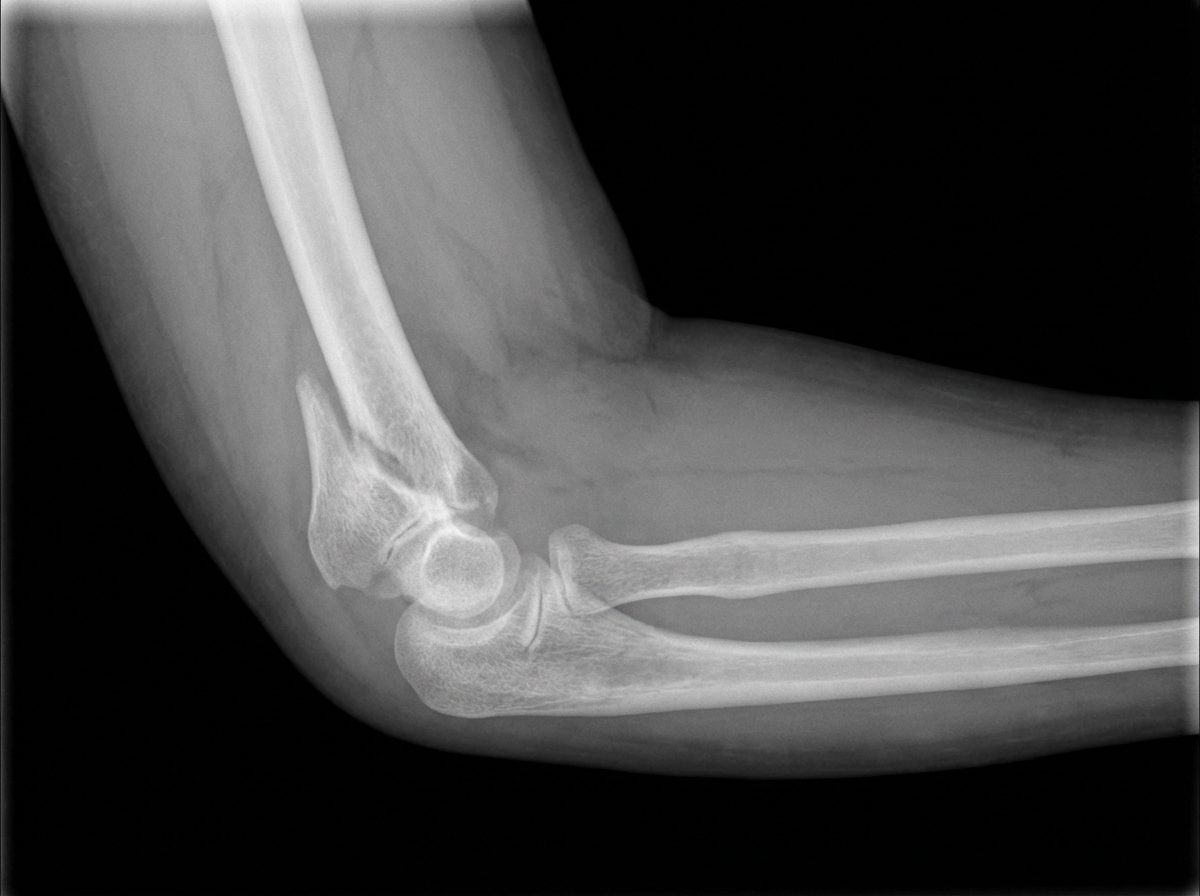
What is the X-ray diagnosis?
A 25-year-old man presents with a blue right arm with absent radial pulse and painful passive finger extension following a supracondylar fracture of the humerus. What condition is he most likely suffering from?
A Tillaux fracture involves which part of the bone?
What is a crescent fracture?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app