
Trauma — MCQs

On this page
Pain around the hip with flexion, adduction, and internal rotation of the lower limb in a young adult after a road traffic accident is suggestive of which of the following conditions?
Which of the following injuries is likely to cause severe vascular damage?
A patient develops compartment syndrome (swelling, pain, and numbness) following manipulation and plaster for a fracture of both bones of the leg. What is the best treatment?
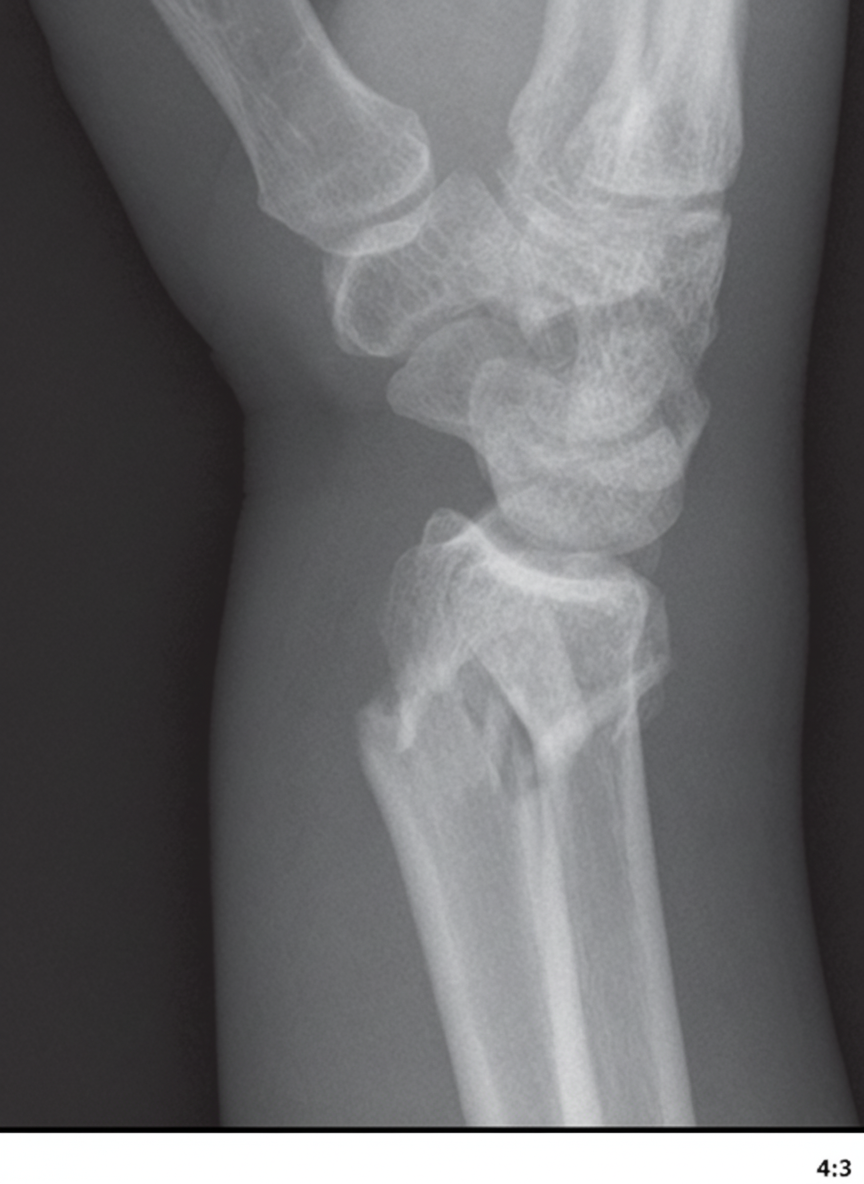
Which of the following complications occurs commonly in the Colles fracture shown in the X-ray, EXCEPT?
What is a comminuted depressed fracture of the lateral tibial condyle classified as?
Garden I fractures are also known as?
In myositis ossificans, where is mature bone typically seen?
What is the commonest complication of extra capsular fracture of the femur?
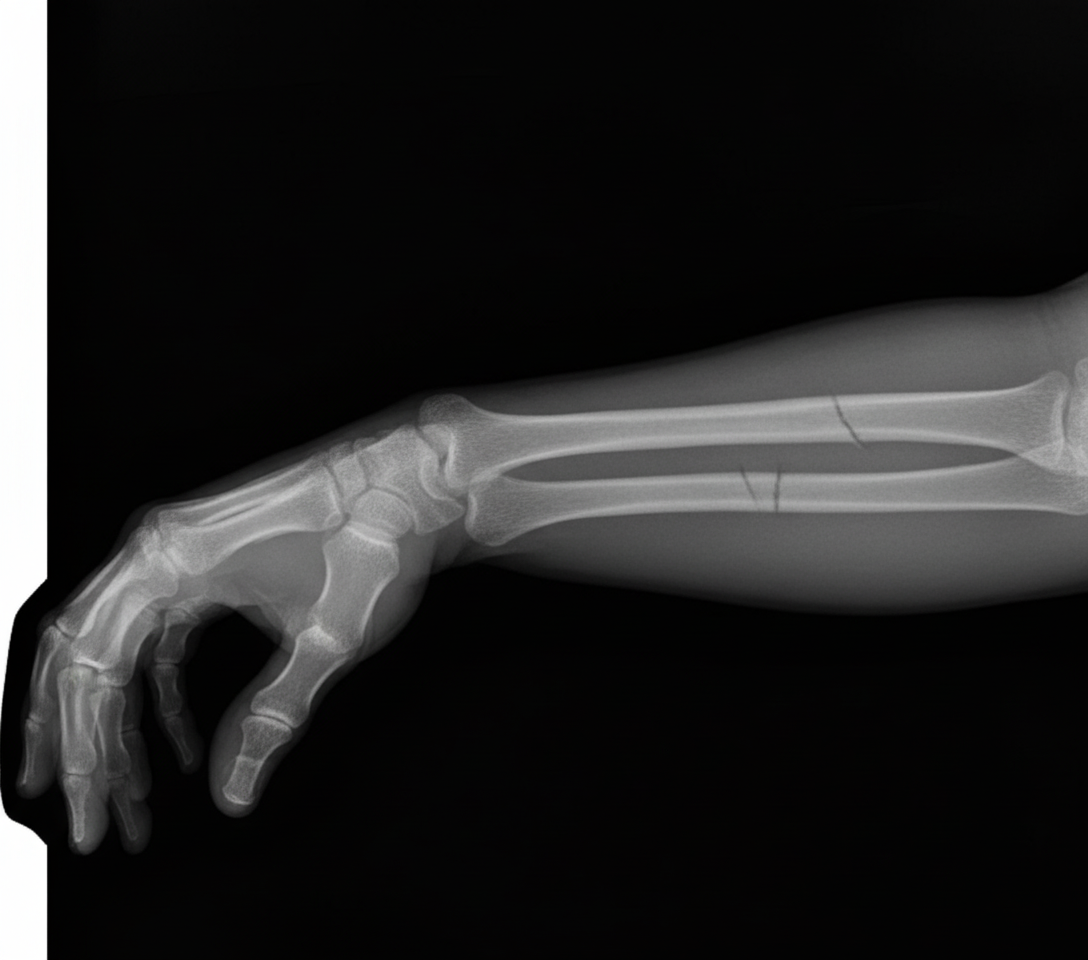
The provided X-ray shows a fracture of which bone?
A 19-year-old man sustains severe lower-extremity trauma, including a femur fracture and a crush injury to his foot. He requires vascular reconstruction of the popliteal artery. On the day after surgery, he becomes dyspneic and hypoxemic and requires intubation and mechanical ventilation. Which of the following is the most likely etiology of his decompensation?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app