
Trauma — MCQs

On this page
A Hill-Sachs lesion in recurrent shoulder dislocation is:
A Bankart's lesion involves which part of the glenoid labrum?
A patient is brought to the emergency following a road traffic accident (dashboard injury). Examination reveals the affected limb is held in flexion, adduction, and internal rotation with apparent shortening. What type of hip dislocation is most likely?
Which of the following is NOT true about calcaneum fracture?
Malgaigne's fracture involves which of the following anatomical structures?
Which of the following statements regarding dislocation of the shoulder is FALSE?
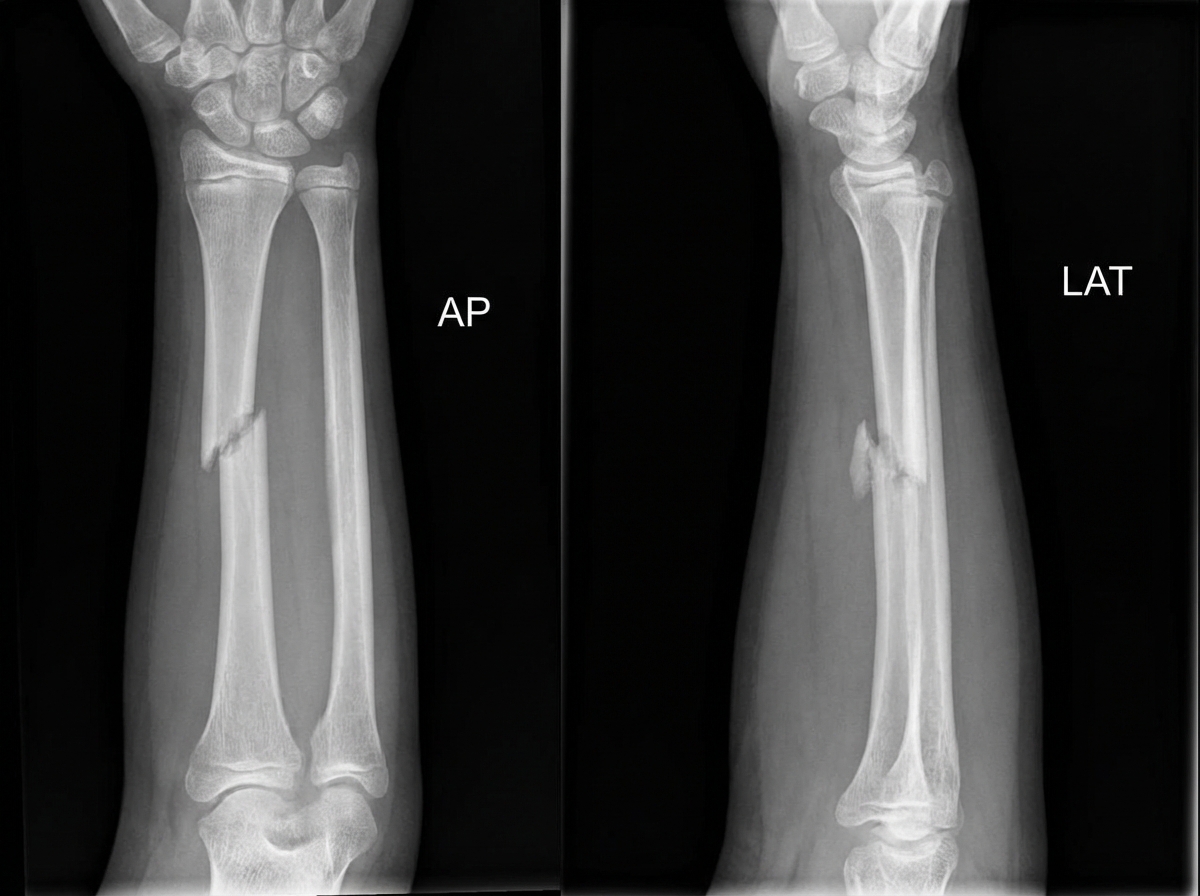
A 13-year-old male presents with forearm pain and deformity after a fall onto his palm. Examination reveals an obvious angulation at the mid-forearm, tenderness over the distal radioulnar joint, and abnormal mobility at the wrist consistent with distal radioulnar joint disruption, with intact finger movement, circulation, and sensation. X-rays of the forearm are obtained. What is the most likely diagnosis?
What type of Monteggia fracture is commonly associated with nerve injuries?
Which of the following is NOT relevant in the management of compartment syndrome?
What is commonly referred to as a Potts fracture?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app