
Trauma — MCQs

On this page
Resolving arthroplasty is seen in which of the following?
Traumatic dislocation of the hip is characterized by which of the following deformities?
Volkmann's ischemic contracture is associated with which of the following conditions?
McMurray's test is positive in which of the following injuries?
Vascular necrosis can be a possible sequelae of fracture of all of the following bones, EXCEPT:
Which of the following tests is positive in anterior dislocation of the shoulder?
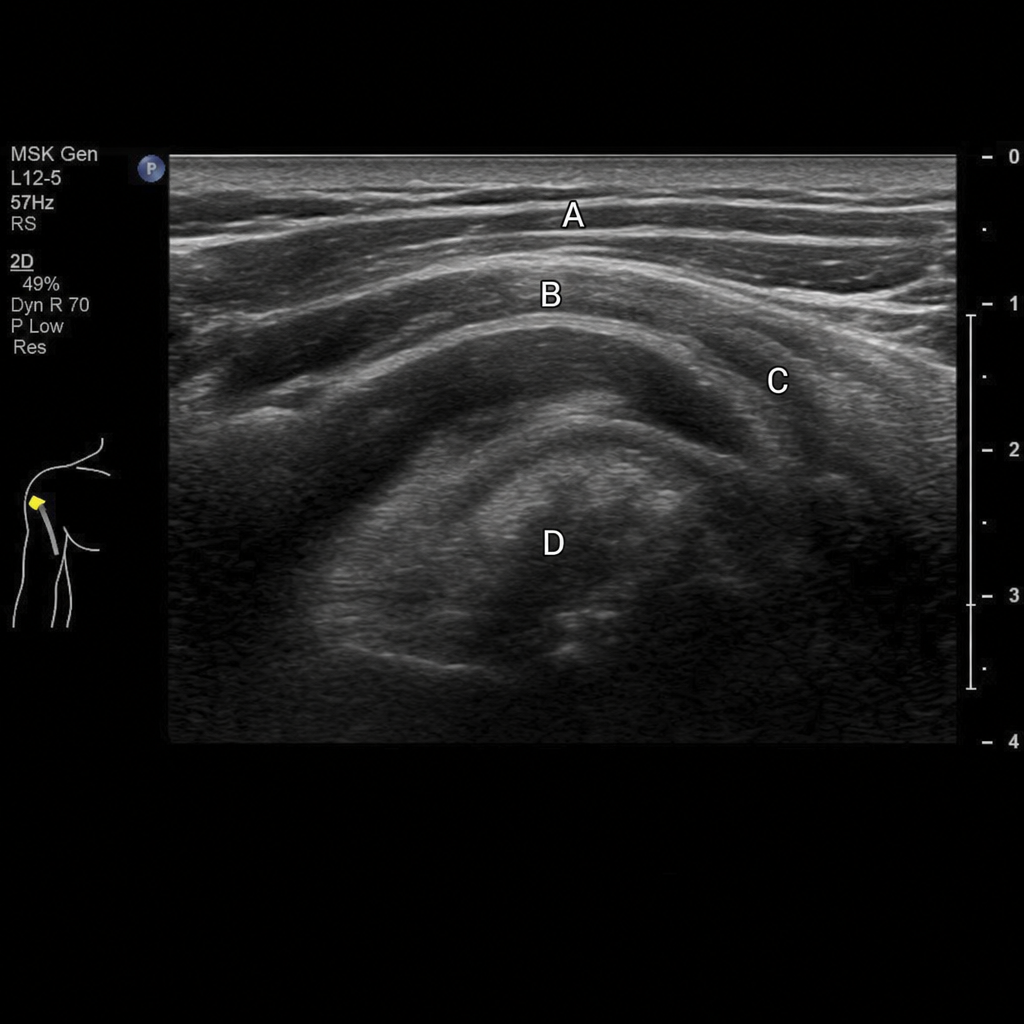
A 40-year-old man presents to the orthopedics emergency with a visible bulge in the upper arm ('Popeye deformity') following lifting a heavy load. Ultrasonography reveals a discontinuity in the proximal tendon with retraction of the muscle belly. Which of the following structures is affected?
Recurrent dislocations are common in which joint?
A compound fracture is initially treated by antibiotics and wound toilet. What is the next appropriate step in management?
A 44-year-old woman suffers a right tibial plateau fracture after a motor vehicle accident. She is neurovascularly intact with soft compartments and has no other significant injuries apart from a minor concussion and several broken ribs. Which of the following, if present, is an indication for operative fixation?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app