
Trauma — MCQs

On this page
All of the following are true about direct trauma, except which of the following?
Which clinical sign is consistently present in all bone fractures?
Which of the following attitudes will be seen in a patient with posterior dislocation of the hip?
Which of the following statements regarding fractures of the lateral condyle of the humerus is false?
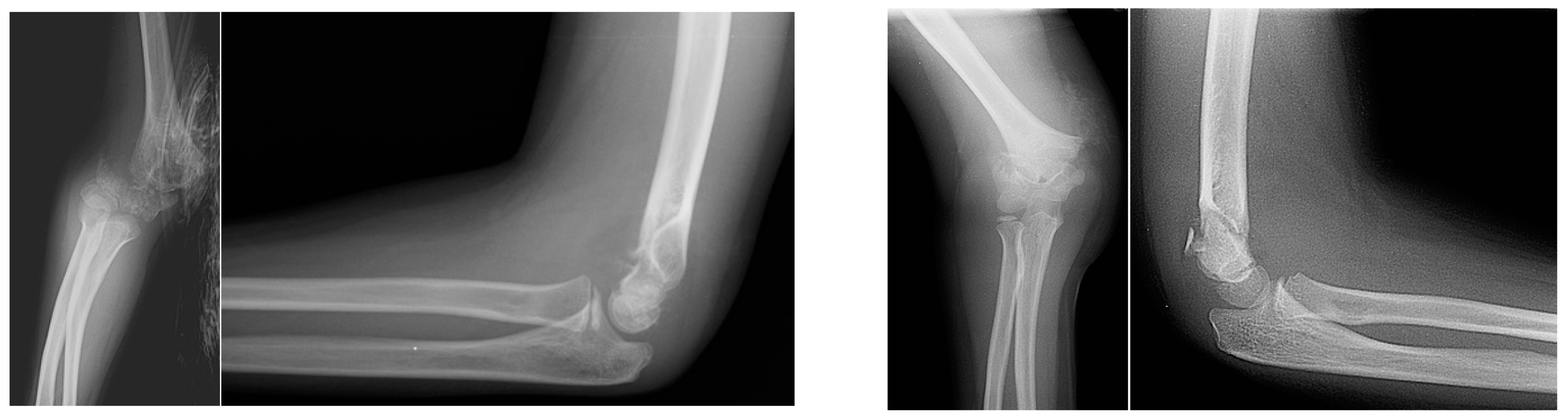
Which of the following classifications is used to assess the fracture shown in the provided image?
A 42-year-old man is brought to the trauma center after a fall from a ladder. Physical examination reveals a slightly deformed left lower extremity with a 0.5 cm soft tissue defect over the anterolateral aspect of his leg. The wound appears relatively clean with no gross contaminants present. Radiographs depict a short oblique proximal one-third diaphyseal tibia fracture. What is his Gustilo open fracture classification grade?
Which of the following statements is false regarding Colles' fracture?
Which of the following is characteristic of a motorcyclist's fracture?
What is the first sign of Volkmann's ischemia?
What is the most appropriate management option for an intra-articular fracture?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app