
Trauma — MCQs

On this page
All of the following are types of avascular non-union except:
What is the best treatment for a fracture of the neck of the femur in a 65-year-old female patient?
Which of the following is/are benefits of immobilization of a fracture?
Which of the following is typically NOT seen in a Colles fracture?
Seddon grading is used for what purpose?
Avascular necrosis is a known complication of which of the following fractures?
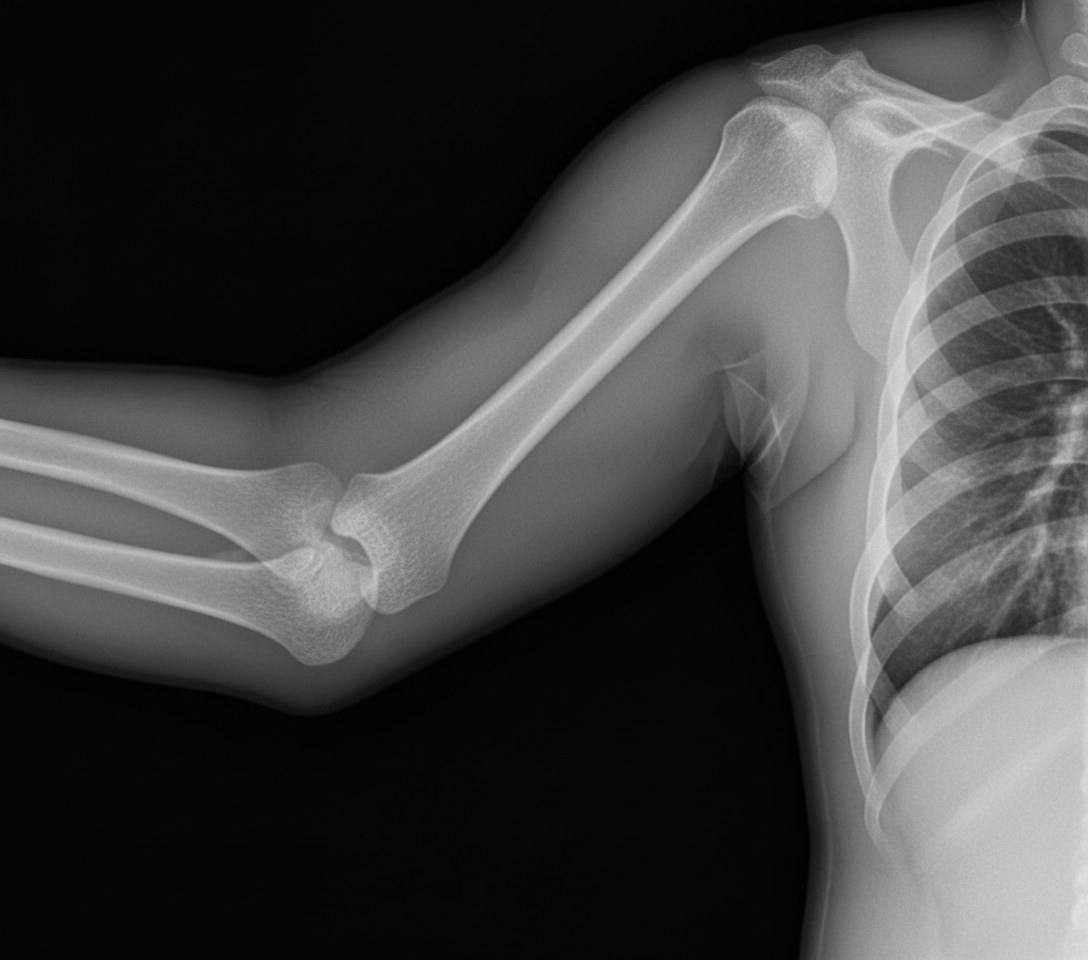
An 18-year-old male presents with a history of trauma. An X-ray is shown below. What is the diagnosis?
A 55-year-old woman presents with a traumatic injury to her right thigh. Which of the following findings is most sensitive for the diagnosis of compartment syndrome?
In lower-third fractures of the shaft of the femur, which displacement does the proximal fragment undergo?
A 25-year-old woman presents to the emergency department following a motor vehicle collision. Radiographic examination reveals a fracture at the spiral groove of the humerus. A cast is applied, and 3 days later, the patient reports severe pain throughout her arm. Physical examination reveals a swollen, pale, and cool arm. The radial pulse is absent, and any movement of the arm causes excruciating pain. Which of the following conditions will most likely characterize these physical examination findings?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app