
Trauma — MCQs

On this page
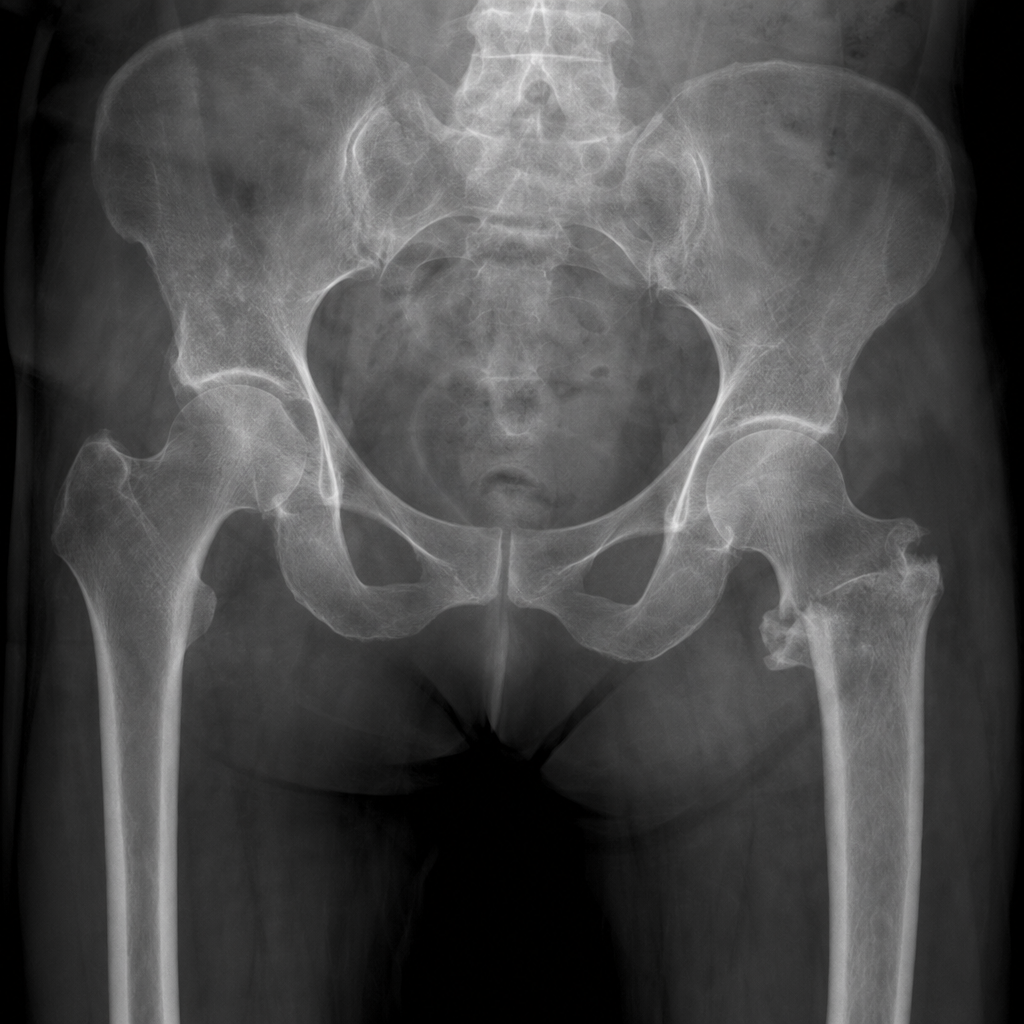
A 28-year-old male is brought to the emergency department following a high -speed motor vehicle collision in which his knee struck the dashboard. On physical examination, the right lower limb is shortened, adducted, and internally rotated. An anteroposte rior X- ray of the pelvis is shown below. Based on the clinical presentation and radiographic findings, what is the most likely diagnosis?
A patient sustained an elbow dislocation that was treated locally. Due to improper healing, the patient later developed a tingling sensation in the palm. Which nerve is most likely involved?
Fracture to the medial epicondyle of the humerus can lead to which of the following nerve injury?
A 28-year-old male with bilateral femoral and tibial fractures and a chest wound presents with unstable blood pressure and tachycardia. After initial stabilization, what is the most appropriate initial management of his long bone fractures?
A proximal humerus fracture is classified using Neer's classification. Which surgical option is most appropriate for a 4-part fracture in a young patient?
In femoral neck fracture management using Garden classification, which treatment is indicated for an elderly patient?
A 30-year-old female post-RTA has persistent pain uncontrolled by analgesics. Compartment pressure is 90 mmHg with absent pulse. What is the treatment?
A 72-year-old osteoporotic woman is brought to the emergency department after a low-energy fall from standing height. Prior to the fall, she was independently mobile in the community without any walking aids, lived alone, and was cognitively intact with no history of dementia or significant cognitive impairment. She has severe right hip pain and is unable to bear weight. On examination, the right lower limb is shortened and externally rotated. Her AP pelvis radiograph confirms a displaced intracapsular (subcapital) femoral neck fracture (Garden Grade IV) as shown in Image 1. She is medically fit for surgery with no significant comorbidities. What is the most appropriate definitive surgical management?
What is the best treatment for an old fracture?
A 40-year-old man presents with a fracture of the shaft of the femur following a road traffic accident. Three days after trauma, he becomes tachypnoeic and develops conjunctival petechiae. What is the most likely diagnosis?
Practice by Chapter
Principles of Fracture Management
Practice Questions
Upper Limb Fractures
Practice Questions
Lower Limb Fractures
Practice Questions
Spinal Trauma
Practice Questions
Pelvic and Acetabular Fractures
Practice Questions
Open Fractures
Practice Questions
Fractures in Children
Practice Questions
Fracture Complications
Practice Questions
Nonunion and Malunion
Practice Questions
Polytrauma Management
Practice Questions
Joint Dislocations
Practice Questions
Soft Tissue Injuries
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app