
Spine Disorders — MCQs

On this page
A 27-year-old woman presents with pain and numbness in her right arm and hand, exacerbated by raising her arm overhead. A provisional diagnosis is made. Which of the following statements is true regarding this condition?
All of the following are radiological features of tuberculosis of the spine except?
What is the most common site for spinal trauma?
A young woman presented with mild quadriparesis following an accident. Her lateral X-ray of the cervical spine revealed a C5-C6 fracture-dislocation. What is the most appropriate line of management?
What is the treatment of choice for a patient with D7-D8 Pott's disease presenting with paraplegia?
Milwaukee brace is used for the management of which condition?
A 25-year-old male presents with a three-month history of lower back pain, following a fall. He reports mild weakness in both lower limbs but can walk without support. He has approximately 30% sensory loss and exhibits bladder symptoms. Physical examination reveals tenderness over D12-L1 vertebrae. X-ray shows paradiscal destruction of vertebrae, and MRI reveals destruction with indentation of the thecal sac. What is the most appropriate management?
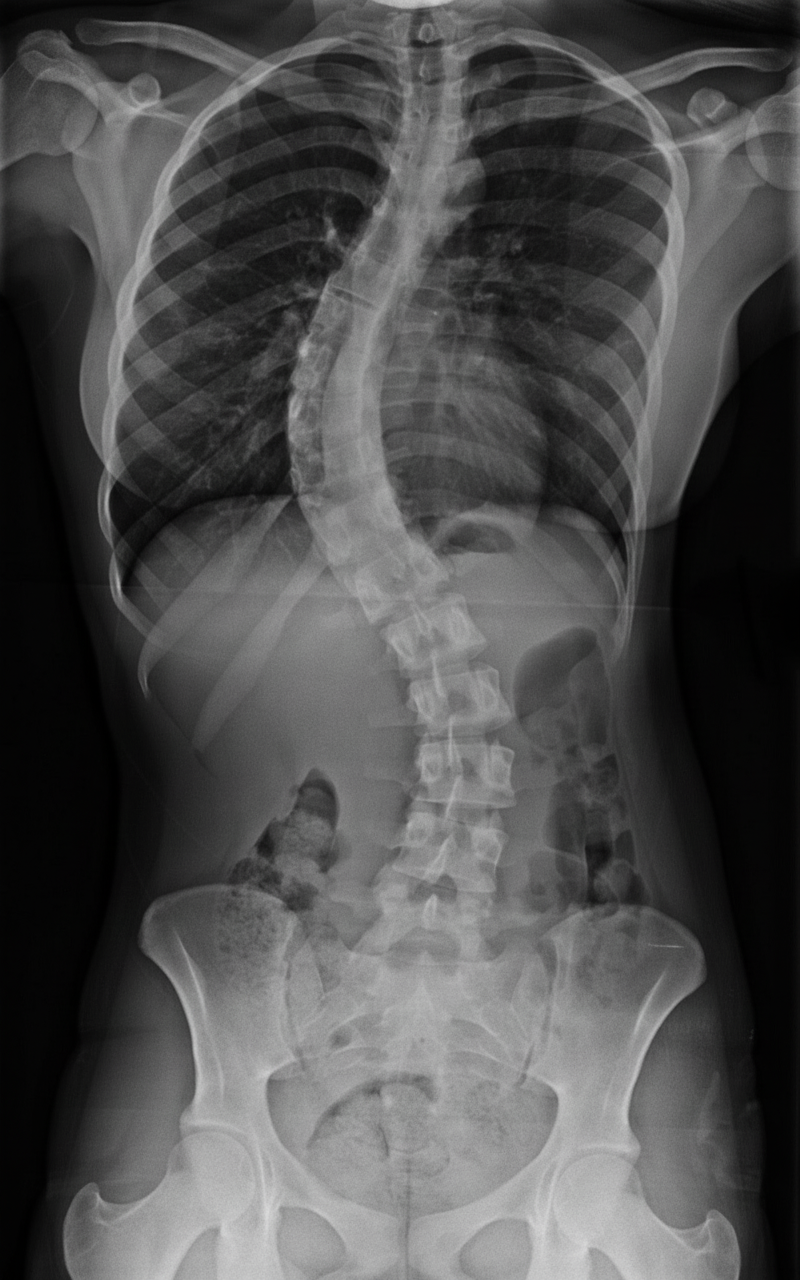
Which of the following spine deformities is being evaluated?
Spondylolysis is more common in which anatomical location?
In a case of tuberculosis of the thoracic spine, what is the earliest sign of cord compression?
Practice by Chapter
Cervical Spine Disorders
Practice Questions
Thoracic Spine Disorders
Practice Questions
Lumbar Spine Disorders
Practice Questions
Intervertebral Disc Disease
Practice Questions
Spinal Stenosis
Practice Questions
Spondylolisthesis
Practice Questions
Spinal Deformities
Practice Questions
Spinal Infections
Practice Questions
Spinal Tumors
Practice Questions
Spinal Cord Injuries
Practice Questions
Minimally Invasive Spine Surgery
Practice Questions
Rehabilitation of Spine Conditions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app