
Spine Disorders — MCQs

On this page
Disc herniation between L4 and L5 involves which nerve root?
What does the return of the bulbocavernous reflex indicate in the context of spinal shock?
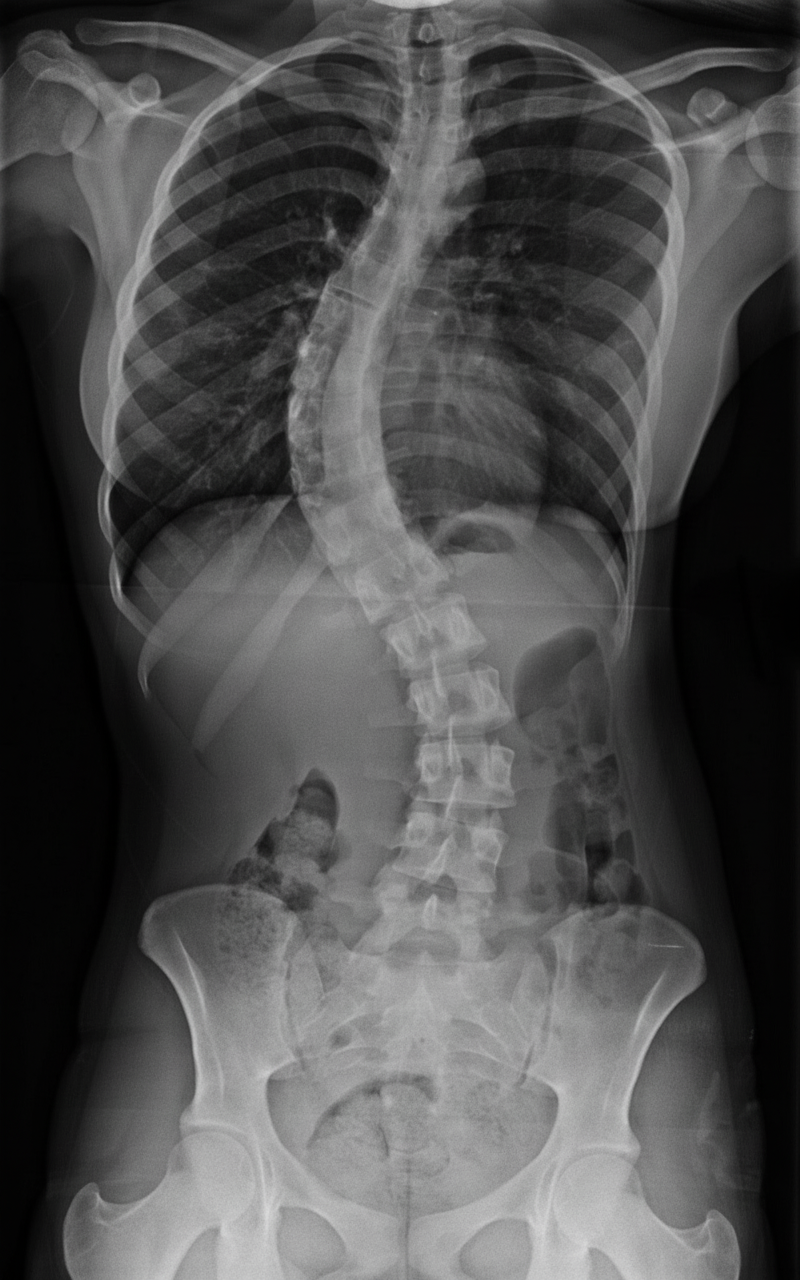
The following X-ray shows a 13-year-old child presenting with difficulty in breathing and gradually developing respiratory compromise. What is the diagnosis?
What is the most common tumor of the spine?
What is the investigation of choice for spinal tuberculosis?
Hangman's fracture is a fracture of which cervical vertebra?
Chance fracture is/are:
What is the likely diagnosis?

What is the most important single special investigation in lumbar disc prolapse?
What is the most common type of spinal cord injury?
Practice by Chapter
Cervical Spine Disorders
Practice Questions
Thoracic Spine Disorders
Practice Questions
Lumbar Spine Disorders
Practice Questions
Intervertebral Disc Disease
Practice Questions
Spinal Stenosis
Practice Questions
Spondylolisthesis
Practice Questions
Spinal Deformities
Practice Questions
Spinal Infections
Practice Questions
Spinal Tumors
Practice Questions
Spinal Cord Injuries
Practice Questions
Minimally Invasive Spine Surgery
Practice Questions
Rehabilitation of Spine Conditions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app