
Spine Disorders — MCQs

On this page
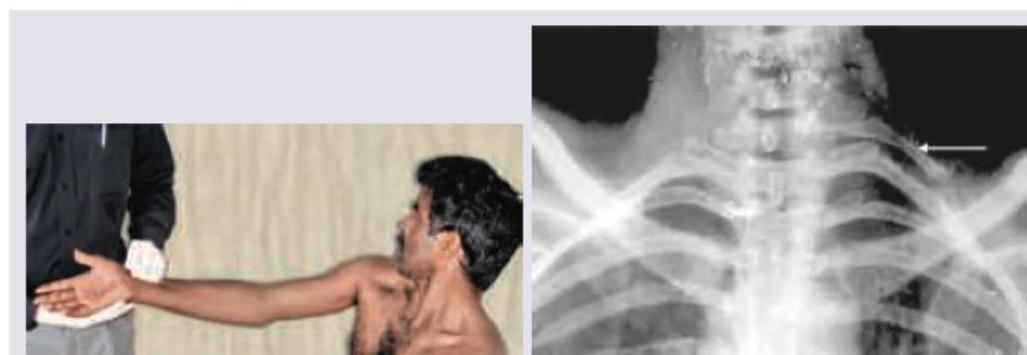
A 40-year-old construction worker presents with pain in the arm on lifting weights. The following test and X-ray of neck was performed. Which is correct about this patient?
Consider the following clinical features : 1. Low back pain 2. Saddle anaesthesia 3. Motor weakness in the lower extremities 4. Variable rectal and urinary symptoms Which of the above features may be present in a patient with Cauda Equina syndrome ?
Hangman's fracture is
Identify the condition shown in the image:
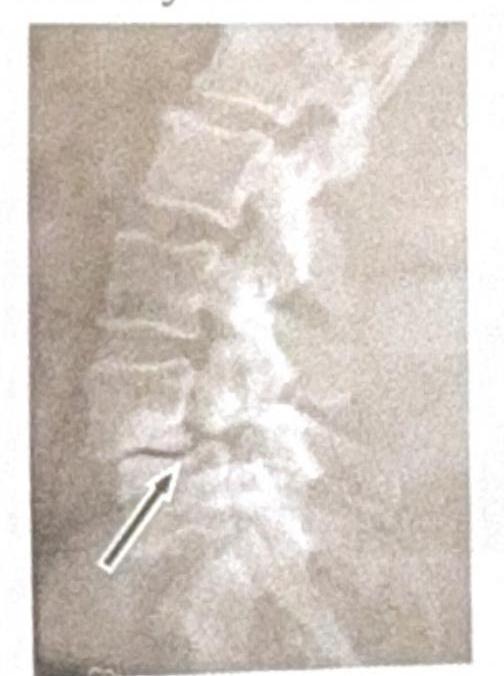
A 35-year-old male presents to the emergency department following a high-speed motor vehicle accident. He complains of severe lower back pain but denies any loss of consciousness or abdominal pain. A lateral X-ray of the lumbar spine is obtained, as shown in the image. The image reveals a horizontal fracture through the vertebral body, extending through the posterior elements. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?

The most common pattern of involvement in Pott's spine is
Most common type of lesion in Pott's spine:
A lady had a trauma to the neck following a high-speed motor vehicle accident with forceful hyperextension. X-ray is attached. What is the diagnosis?

Condition in which there is anterior or posterior displacement of a vertebra in relation to the vertebrae below:
A 47-year-old man awakens with low back pain after a weekend of gardening. He recalls no specific incident of trauma and has never had back pain before. There is no radiation of the pain and no disturbance of normal bowel or bladder function. The ROM of the low back is painful and restricted in all planes, and there is paraspinal tenderness from L2 to L5 on the right. Scoliosis and kyphosis are absent. Findings on straight-leg-raising test are negative, reflexes are active and equal, and the patient can walk on his heels and toes. Findings on x-rays of the lumbar spine are normal. Which is the best treatment?
Practice by Chapter
Cervical Spine Disorders
Practice Questions
Thoracic Spine Disorders
Practice Questions
Lumbar Spine Disorders
Practice Questions
Intervertebral Disc Disease
Practice Questions
Spinal Stenosis
Practice Questions
Spondylolisthesis
Practice Questions
Spinal Deformities
Practice Questions
Spinal Infections
Practice Questions
Spinal Tumors
Practice Questions
Spinal Cord Injuries
Practice Questions
Minimally Invasive Spine Surgery
Practice Questions
Rehabilitation of Spine Conditions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app