
Spine Disorders — MCQs

On this page
Careless handling of a suspected case of cervical spine injury may result in what complication?
A scooter rider is hit from behind and thrown off, landing with their head hitting the kerb. The rider is unresponsive, complains of severe neck pain, and is unable to turn their head. Well-meaning onlookers attempt to sit them up. What is the best course of action in this situation?
What is the most common site of a primary spinal tumor?
In actinomycosis of the spine, the abscess usually erodes:
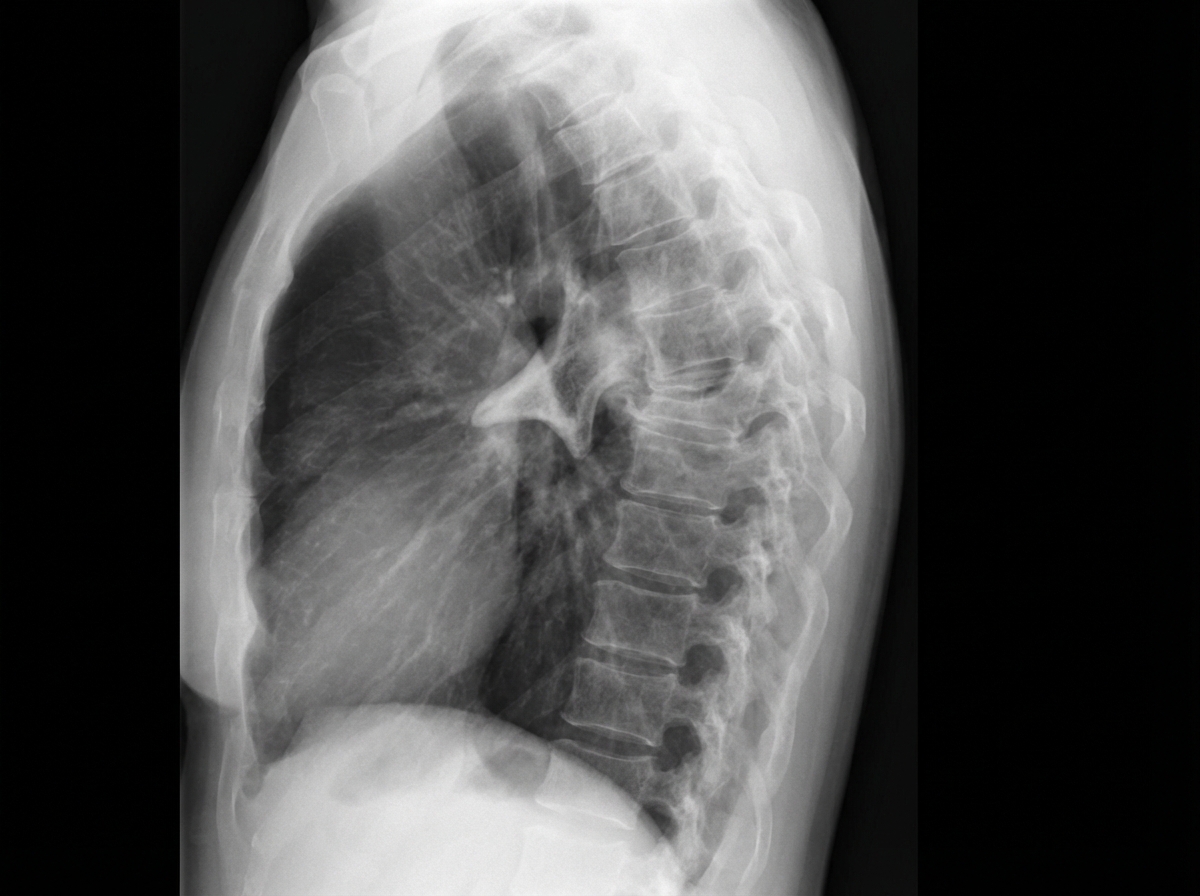
Which of the following spine deformities is seen in the image?
Identify the instrument:

What is the likely diagnosis?

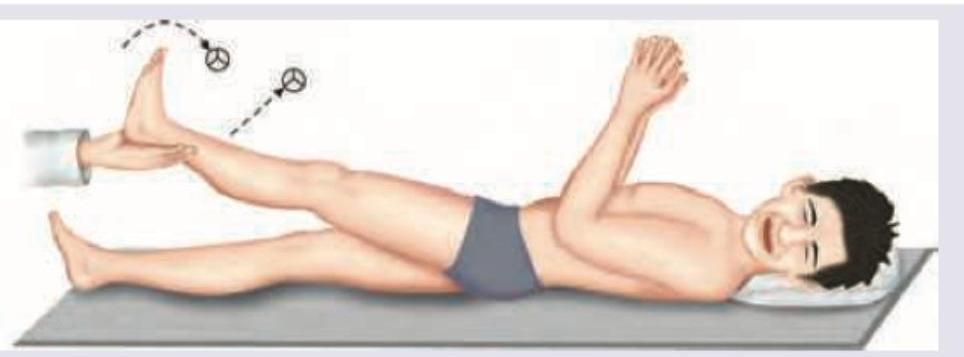
The following test is used to evaluate lumbar disc herniation at which level?
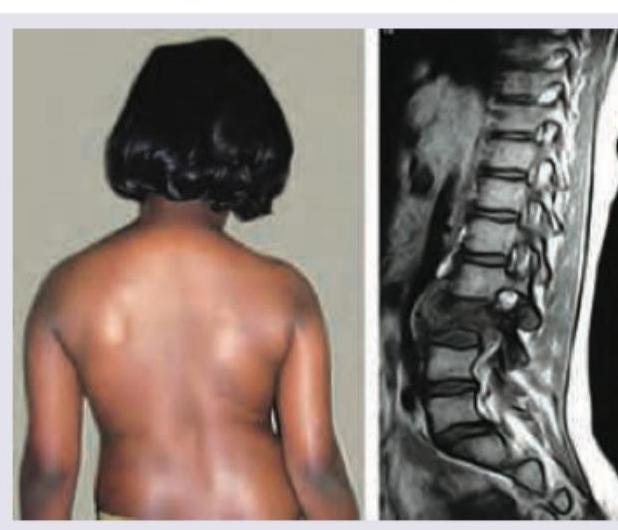
A 10-year-old girl presents with severe back pain for last 4 weeks and deformity of spine. MRI spine was performed and is shown below. All are true about the condition image shown except:
What is the test being performed in the patient?

Practice by Chapter
Cervical Spine Disorders
Practice Questions
Thoracic Spine Disorders
Practice Questions
Lumbar Spine Disorders
Practice Questions
Intervertebral Disc Disease
Practice Questions
Spinal Stenosis
Practice Questions
Spondylolisthesis
Practice Questions
Spinal Deformities
Practice Questions
Spinal Infections
Practice Questions
Spinal Tumors
Practice Questions
Spinal Cord Injuries
Practice Questions
Minimally Invasive Spine Surgery
Practice Questions
Rehabilitation of Spine Conditions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app