
Spine Disorders — MCQs

On this page
A 60-year-old man with treated TB 1 year ago presents with low back pain. MRI spine shows a lesion. What is the most appropriate next investigation?
Which of the following is NOT a clinical feature of Tuberculosis of the Spine?
Flowing wax appearance on anterior and posterior borders of vertebrae with normal intervertebral disc space, occurring due to ligament calcification, is seen in which condition?
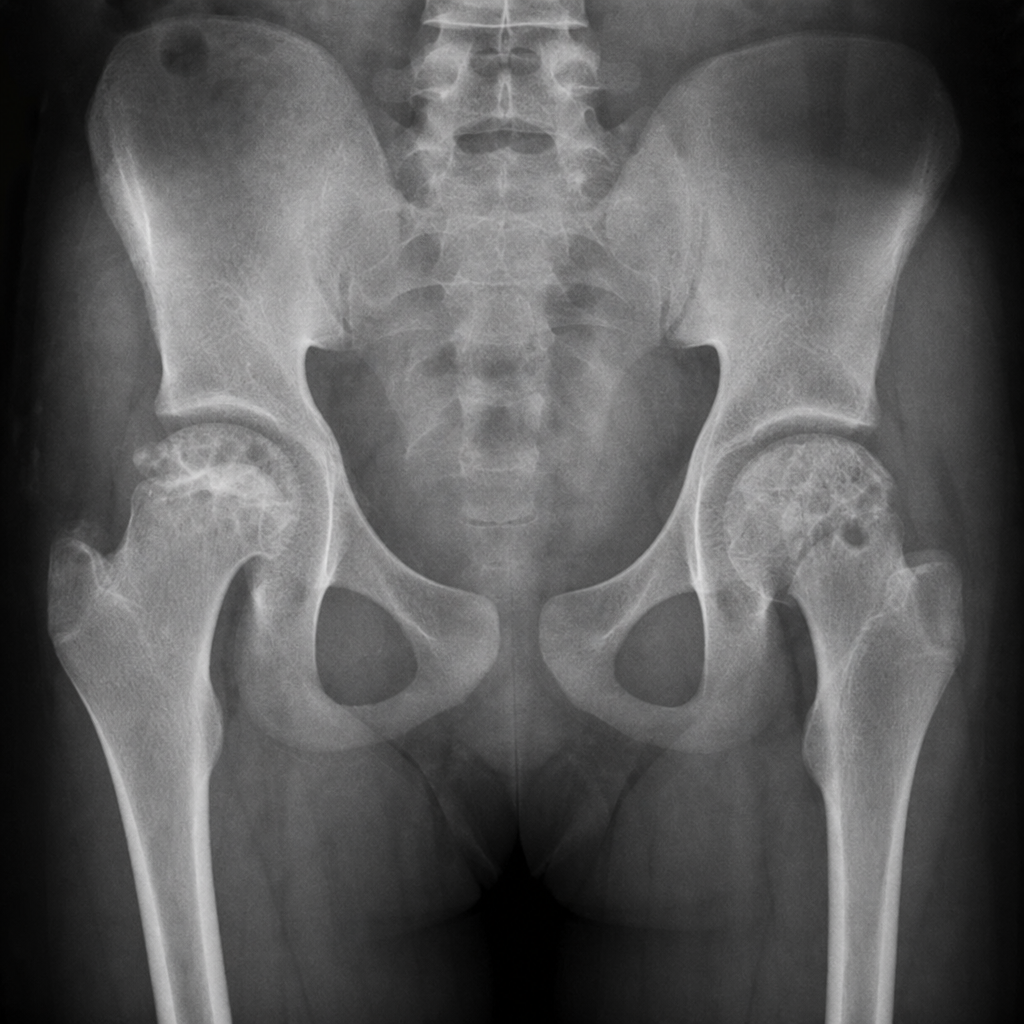
A 45-year-old male presents with bilateral hip pain and restricted range of motion for the past 8 months. He has a history of long-term corticosteroid use for rheumatoid arthritis. The X-ray is shown below. What is the most likely diagnosis?
Which of the following is NOT true regarding Scheuermann's osteochondritis?
Practice by Chapter
Cervical Spine Disorders
Practice Questions
Thoracic Spine Disorders
Practice Questions
Lumbar Spine Disorders
Practice Questions
Intervertebral Disc Disease
Practice Questions
Spinal Stenosis
Practice Questions
Spondylolisthesis
Practice Questions
Spinal Deformities
Practice Questions
Spinal Infections
Practice Questions
Spinal Tumors
Practice Questions
Spinal Cord Injuries
Practice Questions
Minimally Invasive Spine Surgery
Practice Questions
Rehabilitation of Spine Conditions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app