
Arthrology and Infections — MCQs

On this page
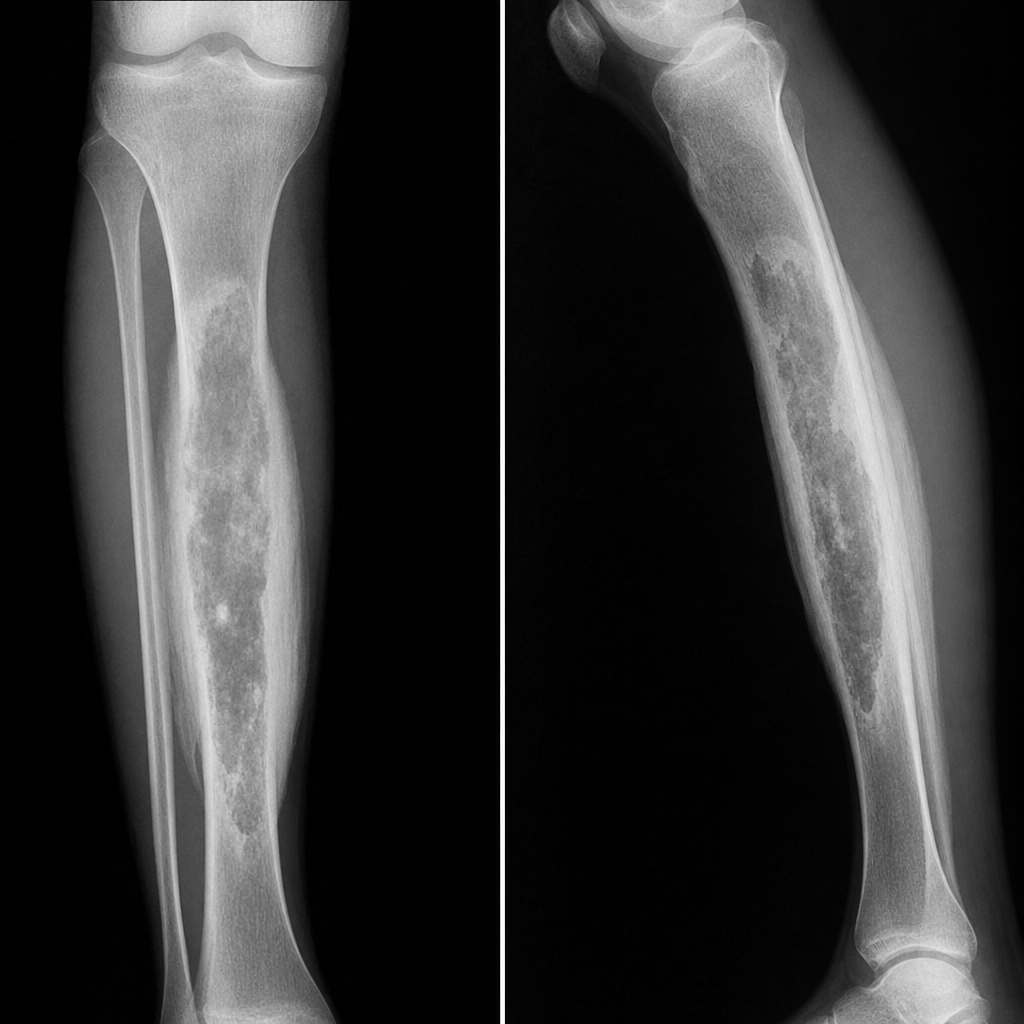
A 35-year-old patient has a history of RTA 2 years ago with an open fracture that required surgical fixation. He now presents with pain, swelling, and a draining sinus at the same site. What will be the diagnosis based on the provided X-ray features?
A 20 year old male presents with history of gradual onset pain and swelling in left knee since 6 months. Now since last 1 month patient has started limping while walking and also has flexion deformity of knee. Ultrasonography shows presence of synovial thickening. What is the most probable diagnosis?
X-ray appearance of sequestrum?
First radiological sign for active tubercular arthritis is?
Deformity of hip in stage of tubercular synovitis?
Most common joint involved in septic arthritis:
During performing a total hip replacement, the surgeon found destruction of the articular cartilage and multiple wedge-shaped subchondral depressions. What is this called?
How is Brodie's abscess classified?
What is another name for ischial bursitis?
Which of the following is an orthopedic emergency?
Practice by Chapter
Septic Arthritis
Practice Questions
Osteomyelitis
Practice Questions
Tuberculosis of Bones and Joints
Practice Questions
Fungal and Parasitic Infections
Practice Questions
Diabetic Foot Infections
Practice Questions
Prosthetic Joint Infections
Practice Questions
Reactive Arthritis
Practice Questions
Management of Joint Infections
Practice Questions
Prevention of Orthopaedic Infections
Practice Questions
Biofilms in Orthopaedic Infections
Practice Questions
Antibiotic Prophylaxis
Practice Questions
Implant-Related Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app