
Arthrology and Infections — MCQs

On this page
All are features of a haemophilic knee joint, EXCEPT?
Fibrous ankylosis is caused by which of the following?
What is the radiographic appearance of dead bone on an X-ray?
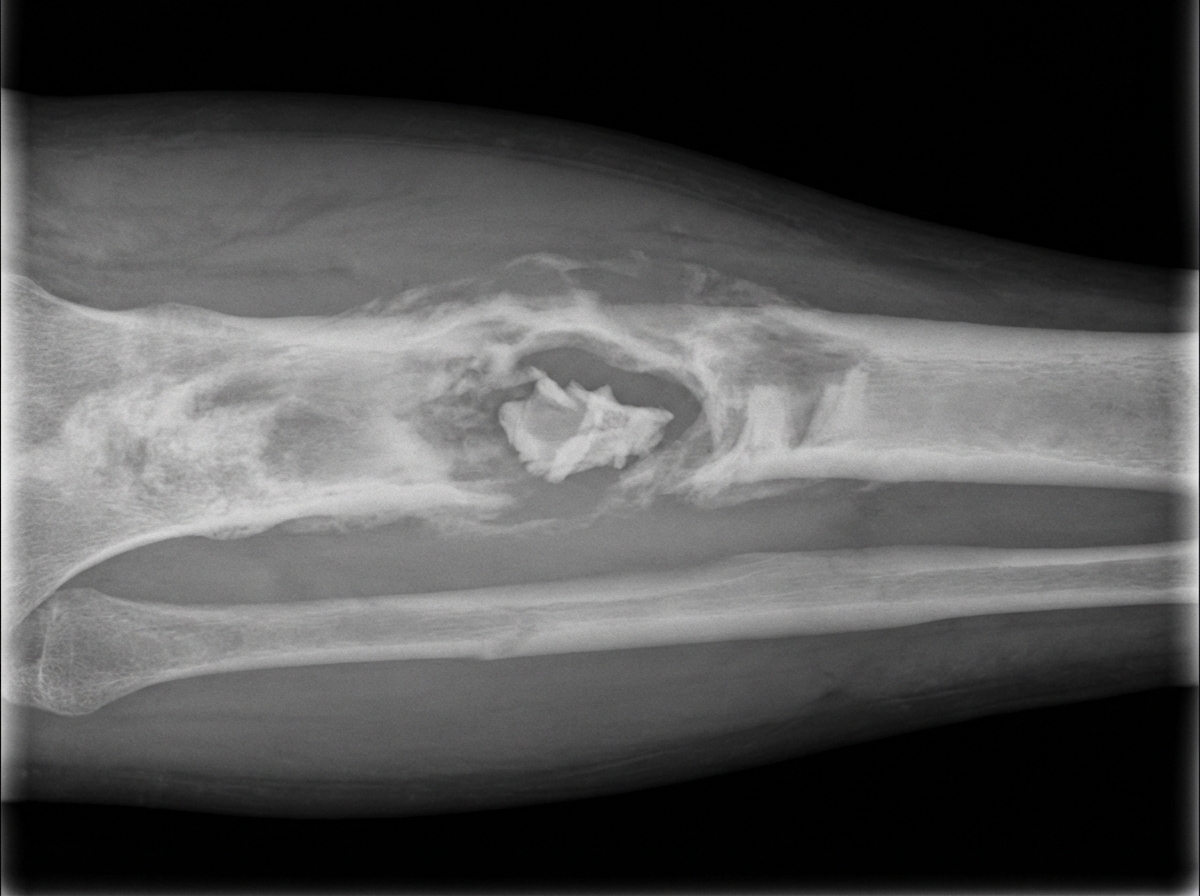
Brodie's abscess is the terminology for:
What is the earliest site of bone involvement in hematogenous osteomyelitis?
A child presents with a swollen, painful knee and high fever, with no history of trauma. Acute osteomyelitis is suspected. Which part of the bone is earliest involved in hematogenous osteomyelitis?
Charcot's joint is another name for a joint affected by which condition?
Monoarticular joint involvement is seen in which of the following?
Which of the following statements is FALSE regarding the given lesion (Garré's chronic sclerosing osteomyelitis of long bones)?
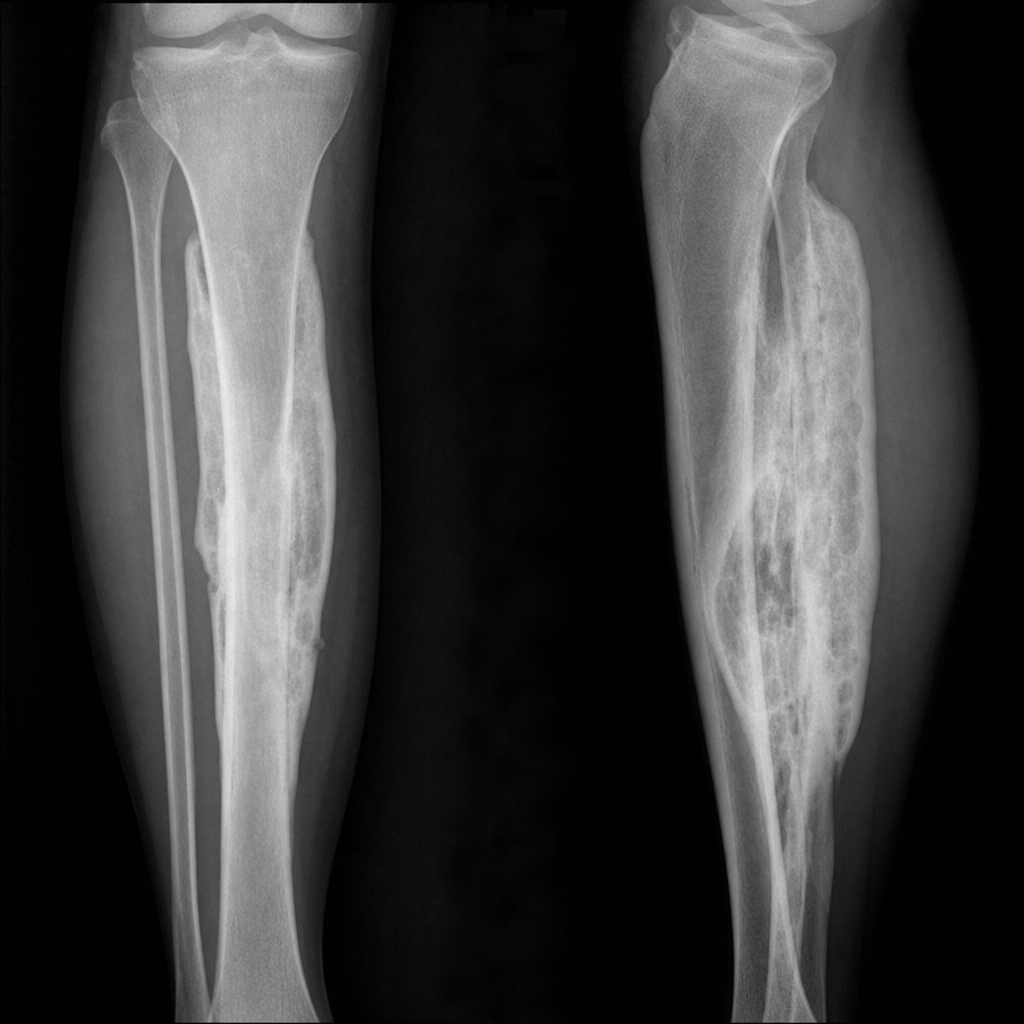
A patient has a history of similar symptoms at the same site two years ago, developing pain and swelling. X-ray shows the following features. What is the diagnosis?
Practice by Chapter
Septic Arthritis
Practice Questions
Osteomyelitis
Practice Questions
Tuberculosis of Bones and Joints
Practice Questions
Fungal and Parasitic Infections
Practice Questions
Diabetic Foot Infections
Practice Questions
Prosthetic Joint Infections
Practice Questions
Reactive Arthritis
Practice Questions
Management of Joint Infections
Practice Questions
Prevention of Orthopaedic Infections
Practice Questions
Biofilms in Orthopaedic Infections
Practice Questions
Antibiotic Prophylaxis
Practice Questions
Implant-Related Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app